


ISSN: 0973-7510
E-ISSN: 2581-690X
Rheumatoid arthritis (RA) is a systemic inflammatory disease with chronic nature of joints related to autoimmunity. Vitamin D was found to modulate cell growth, function of immune cells and anti-inflammatory action. The aims of that study were to investigate serum level of vitamin D and some cytokines and to identify the correlation between vitamin D and these cytokines in RA. Totally 40 RA patients without vitamin D supplement were involved in this study. Serum level of vitamin D, interleukin-6 (IL-6), IL-10, IL-35, C-reactive protein (CRP) and tumor necrosis factor α (TNF-α), all of them were measure in all patients by enzyme-linked immunosorbent assay (ELISA). Patients were classified according to Vitamin D levels into two groups; RA patients with Vit. D deficiency (n=25) and RA patients with Vit. D sufficiency (n=15). IL-6 was lower significantly (P = 0.03) in RA patients with Vit. D sufficiency than RA patients with Vit. D deficiency. IL-10 and IL-35 were higher significantly (P = 0.0234, P = 0.0356 respectively) in RA patients with Vit. D sufficiency than RA patients with Vit. D deficiency. Vit. D was significantly positively correlated with both IL-10 (r = 0.4516, P = 0.0034) and IL-35 (r = 0.3424, P = 0.0329) and negatively correlated with IL-6 (r = -0.3188, P = 0.0479). Sufficient serum level of Vit. D is correlated with higher level of anti-inflammatory cytokines (IL-10 and IL-35) and lower level of IL-6. This support the immunomodulatory effect of Vit. D in RA.
Vitamin D, Rheumatoid Arthritis, pro-inflammatory, anti-inflammatory, cytokines
Rheumatoid arthritis (RA) is a systemic inflammatory disease with chronic nature of joints related to autoimmunity. RA could lead to accumulative joint damage and thus permanent disability1.
Even though vitamin D upholds calcium absorption from the gut and sustains sufficient serum levels of calcium and phosphate, it also essential for the vigor of both osteoblasts and osteoclasts2,3. In addition, vitamin D was found to modulate cell growth, the function of immune cells and anti-inflammatory action. Also modulate in part numerous genes responsible for cell proliferation, differentiation and also apoptosis4,5.
While vitamin D has been proven to persuade anti-inflammatory activity either paracrine or intacrine, the precise pathway by which vitamin D get into different types of immune cells and express 1a-hydroxylase is still ambiguous6.
The immune-modulatory impact of vitamin D are proved by the presence of vitamin D receptors (VDRs) on peripheral mononuclear blood cells7,8. That, vitamin D leads to down-regulation of numerous kinds of immune cells comprising tumor necrosis factor-alpha (TNF-a), antigen-presenting cells, interferon gamma, T-cell proliferation and the cytokine IL-29,10. Many studies made a relation among vitamin D deficiency and various autoimmune diseases such as systemic lupus erythematous (SLE), type 1 diabetes mellitus and RA11-14. A recent study reported that, vitamin D significantly inverse correlated with the activity of RA disease15.
A broad range of many types of cells express vitamin D receptors thus, they could respond to vitamin D16, such as chondrocytes and synoviocytes in the joints of RA patients. Moreover, genetic variation in VDR gene had been considered as a risk factor for RA17-20.
Also vitamin D could down regulate B-cells proliferation and differentiation by apoptotic techniques in activated B-cells21, and consecutively suppress the proliferation of T-cells and inhibits the production of TNF-𝛼, INF-𝛾 and IL-2 cytokines22.
Many studies have focused to discover the influence of vitamin D therapy on TNF-𝛼 synthesis and have been summarized to the presence of an inverse correlation between them23.
TNF-a is a prevalent pro-inflammatory cytokine in RA pathogenesis and is highly expressed the synovial fluid. Selective blockage of TNF-a leads to relieve of RA progression24,25.
IL-6 plays a crucial role in RA pathogenesis, thus it promotes autoantibodies production and regulation of TH- cells differentiation26. Also its signaling cascades trigger bone erosion, joint inflammation27, acute phase response, synovial fibroblasts proliferation and promote hematopoietic cells28.
Vitamin D sufficient level have been related to reduced serum IL-629 by the mastery of vitamin D to suppress the synthesis of IL-6 transcription thru the stimulation of MAPK phosphatase-1 (MKP1) which leads to p38 inhibition by its dephosphorelation. The dephosphorelated p38 resulting in down regulation of IL-6 gene transcription30.
On the other side, vitamin D could up-regulate the anti-inflammatory cytokines as IL-1031 and IL-432 and. This was proven by in vitro study that reported vitamin D3 therapy could enhance the production of Th2 lymphocytes which in turn amplified the manufacture of IL-4, IL-5, and IL-1033. IL-10 is a sturdy anti-inflammatory cytokine and plays a vital role in relieving RA signs34 through inhibiting both the infiltration and activation of neutrophils in the synovial fluids35, constraining pro-inflammatory cytokines expression as TNF-a36, pointing macrophages to polarize into an M2 phenotype. In vitro study reported that, nullification of IL-10 activity in RA synovial membrane cultures resulted in augmented level of pro-inflammatory cytokines like IL-1β and TNF36.
IL- 35 is a heterodimeric cytokine and it is one of IL-12 family37. IL-35 could down regulation T-cell proliferation and induce regulatory T cells (iTr35) as a result of the creation of pSTAT1:pSTAT4 heterodimers38. IL-35 chiefly released by Treg cells39, however a recent study reported that, IL-35 is also released by regulatory B cells (Breg)40,41.
Several studies have revealed the anti-inflammatory properties of IL-35, in which it could promote Treg-cells and deter Th17 cells in many experimental inflammatory diseases models such as collagen induced arthritis (CIA)42, also in vitro treatment with IL-35 inhibited fibroblast-like synoviocytes (FLS) proliferation and promoted its apoptosis in a dose-dependent manner cultured from CIA mice43. Furthermore, IL-35 could suppress the expression of vascular endothelial growth factor (VEGF) and repressed angiogenesis in CIA mice model thus made the severe synovitis much better44.
The aims of that study were to investigate the serum level of vitamin D and some cytokines and identify the correlation between vitamin D and these cytokines and the correlation among the cytokines.
Patients
That study was conducted during 2019 after approval of the ethical committee of the university hospital (Ref number 17100135). A written informed consent was obtained after discussing a detailed description of the study with the patient. Patients were informed that they can withdraw their consent to participate at any time. The work was done in agreement with the Declaration of Helsinki.
According to ACR/EULAR criteria for classification of RA disease(45), Forty patients attending routinely outpatient clinic of Rheumatology, Department of Rehabilitation and Physical Medicine, Assiut University Hospital, Egypt diagnosed with RA were selected in this study. All the recruited patients underwent a thorough clinical assessment to detect the clinical activity of the disease using Rheumatoid disease activity score DAS28, patients should have a score less than 2.6 for at least 3 months prior enrollment to the study46.
In addition, all patients were receiving Methotrexate and Leflunomide. The exclusion criteria included: active RA (DAS>2.6), patients receive vitamin D supplement, patients receive corticosteroids, Patients with inflammatory bowel disease, patients with any other autoimmune diseases or patients aged younger than 15 years.
Patients are classified into 2 groups according vitamin D level; RA patients 25-OH Vit. D deficient and RA patients 25-OH Vit. D sufficient.
Healthy volunteers
Forty healthy volunteers without rheumatoid arthritis, inflammatory bowel disease or any other autoimmune disease have been recruited in this study to measure their serum 25-OH Vitamin D only.
Serum samples
Five millimeters of fasting venous blood sample were collected from the selected RA patients and healthy volunteers in a sterile plain tube and left to clot. Then, centrifuged. Each serum sample was distributed in 5 cryogenic vials and deposited at -80°C for extra analysis.
Determination of total 25-OH Vitamin D (25-OH Vit. D)
Serum concentration (ng/mL) of total 25-OH Vit. D was determined for both RA patients and healthy volunteers by enzyme immunoassay by following the manufacturer protocol of Epitope Diagnostic kit (San Diego, CA: 92121, USA). According to manufacturer guidelines vitamin D deficiency will be fewer than 20 ng/mL and optimal vitamin D level will be 20-70 ng/mL.
Measurement of C-reactive protein (CRP)
Serum concentration (ng/mL) was measured for RA patients according to manufacturer protocol. HIGH SENSITIVITY C-REACTIVE PROTEIN (hs- CRP) ELISA KIT of Diagnostic Biochem Canada (CA: CAN-CRP-4360, London, Ontario, Canada N6M 1A1) was used. The sensitivity of the ELISA kit was 10 ng/mL.
Assay of IL-6, IL-10 and IL-35 cytokines and tumor necrosis factor a (TNF-a)
Serum concentration (ng/L) for IL-6, IL-10 and TNF-a and (pg/ml) for IL-35 was measured for RA patients according the manufacturer protocol. Human Interleukin ELISA kits of SinoGeneClon Biotech ((CA: SG-10267) for IL-6, (CA: SG-10271) for IL-10, (CA: SG-10297) for IL-35 and (CA: SG-10127) for TNF-a) were used. The sensitivity of the ELISA kits was 0.05 ng/L, 1.0 ng/L, 15.6 pg/ml and 2 ng/L for IL-6, IL-10, IL-35 and TNF-a respectively. the detection range was 0.2 ng/L – 8 ng/L, 10 ng/L – 300 ng/L, 150 pg/ml – 4800 pg/ml and 7 ng/L – 400 ng/L for IL-6, IL-10, IL-35 and TNF-a respectively.
Statistical analysis
All data were documented on Microsoft Excel. All statistical analyses were carried out by means of the program GraphPad Prism version 8.0.1 (244) (San Diego, CA, USA). All results are informed as mean together with standard deviation (SD).
Demographic data
Totally 80 persons, of them 40 patients (38 females and 2 males) from 2 governorates; Assiut and Sohage, upper Egypt, Egypt. The mean age for RA patients was 43.23 ± 9.037 (Table 2). There was no statistically significant difference among the two RA groups within age. All patients with active RA according to diagnosis based on ACR/EULAR criteria. It was obvious from the rate of patient’s admission to outpatient clinic, the RA is prevalent more among women than among men (Table 2). All the healthy volunteers from Assiut governorate.
Total serum 25-OH Vitamin D (25-OH Vit. D) level and correlation with other parameters
According to manufacture guidelines, patients having vitamin D level < 20 ng/mL are considered deficient in 25-OH Vit. D and those having vitamin D level ≥ 20 ng/mL are considered normal in 25-OH Vit. D. Accordingly, 25 patients were deficient in 25-OH Vit. D level with mean ± SD 12.93 ± 4.753, whereas only 15 patients were with normal 25-OH Vit. D level with 41.40 ± 14.77 (Table 2). Thus patients are classified into 2 groups; RA patients 25-OH Vit. D deficient and RA patients 25-OH Vit. D sufficient. The variance between the two groups were statistically significant with P value < 0.0001 (Table 2) (Fig. 1). Also for healthy volunteers 18 persons were found to be sufficient in 25-OH Vit. D level with mean ± SD 27.12 ± 3.705, however 22persons were found to be deficient in 25-OH Vit. D level with mean ± SD 18.50 ± 1.017. the difference in total serum 25-OH Vit. D level between RA patients and healthy volunteers were significant with P value 0.0193 (Table 1). Serum 25-OH Vit. D level correlated significantly with the serum level of both IL-10 (r = 0.4516, P = 0.0034) and IL-35 (r = 0.3424, P = 0.0329) (Table 3) (Fig. 2). Moreover, serum 25-OH Vit. D level negatively correlated significantly with the serum level of IL-6 (r = -0.3188, P = 0.0479). While, 25-OH Vit. D did not correlate with both TNF-a (r = -0.1141, P = 0.4834) and c-reactive protein (CRP) (r = 0.009931, P = 0.9515) (Table 3) (Fig. 2).
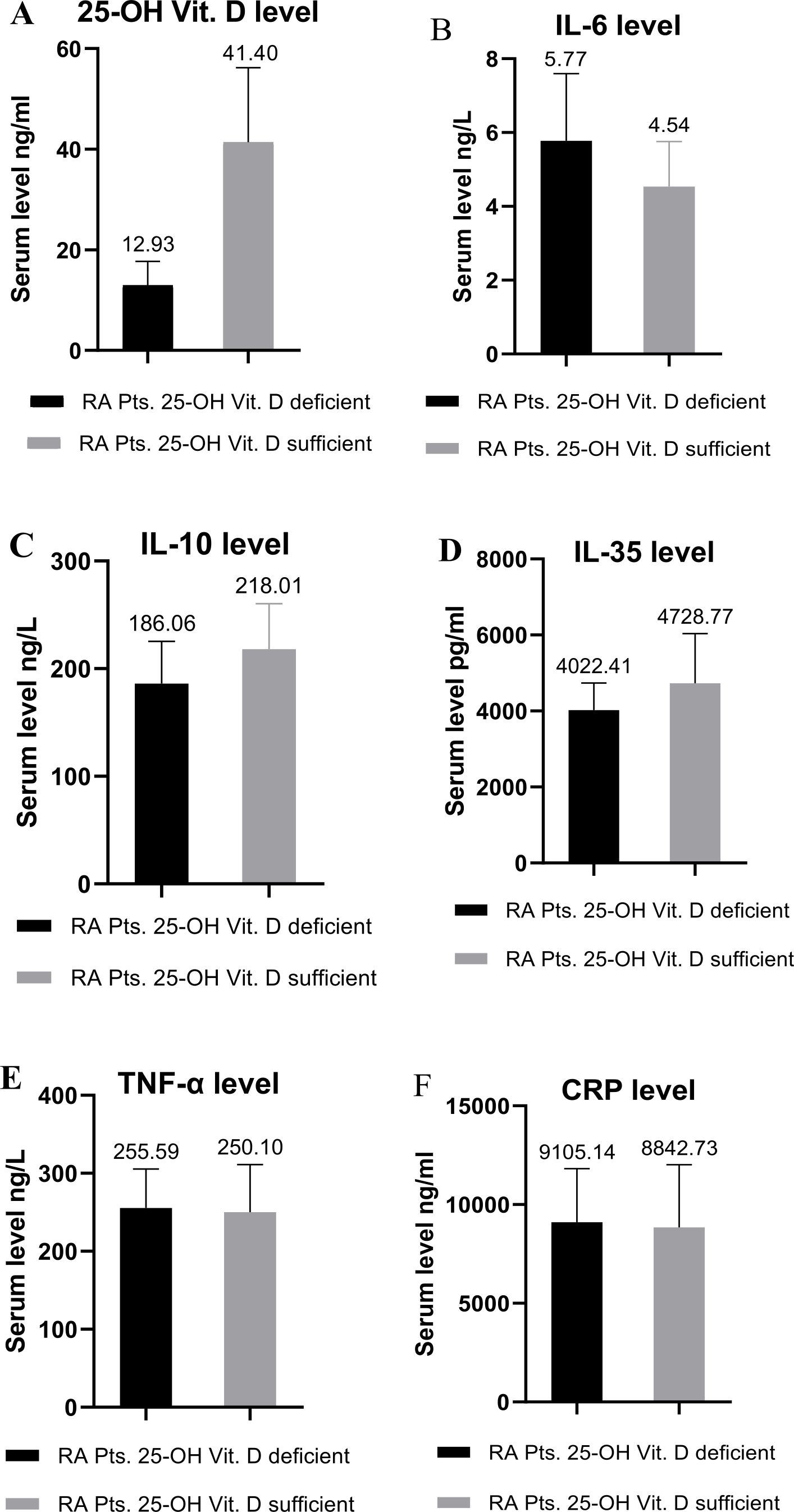
Fig. 1. Baseline features of RA patients with Vit. D deficiency and RA patients with Vit. D sufficiency. (A), IL-6 (B), IL-10 (C), IL-35 (D), TNF-α (E) and finally CRP (F).
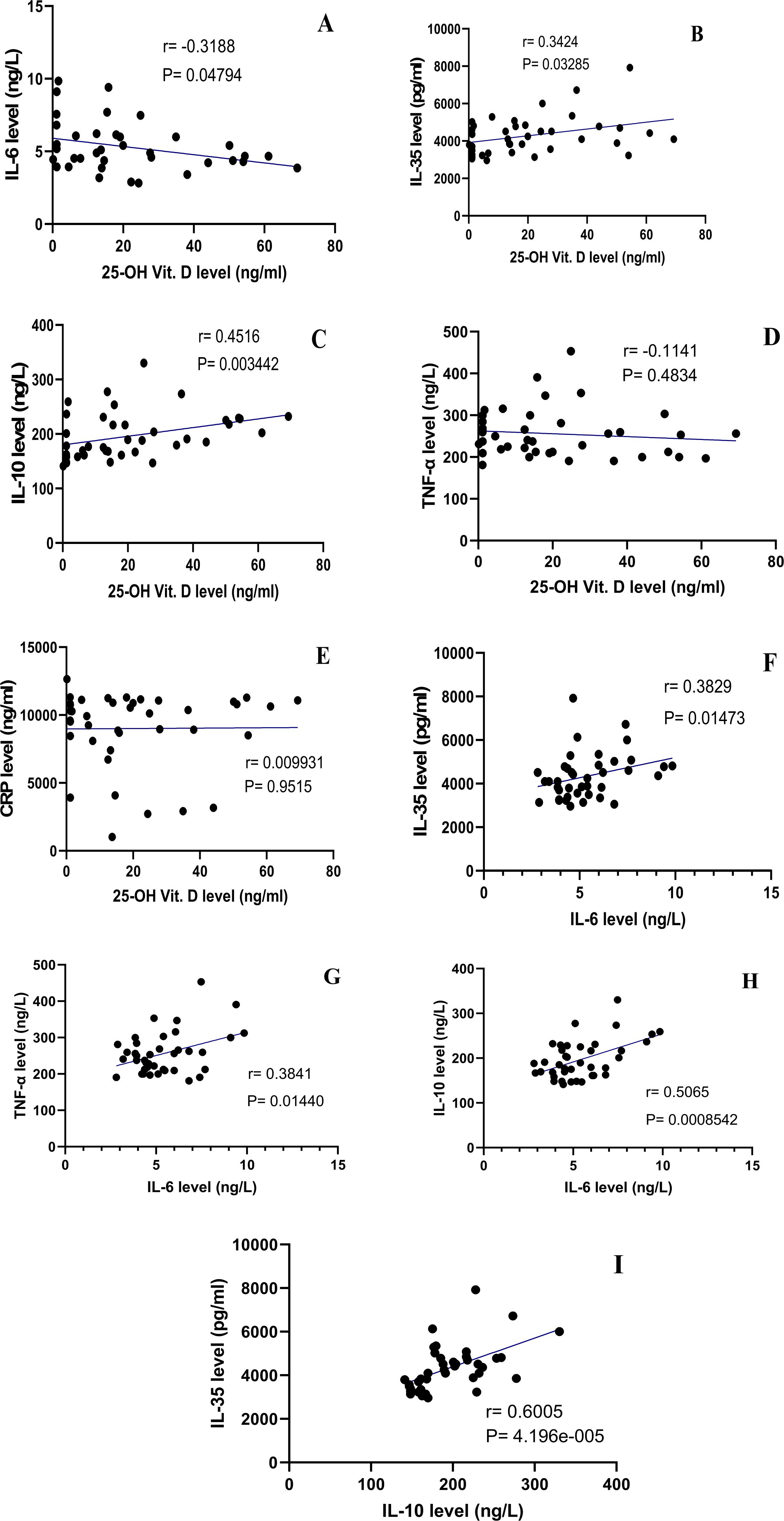
Fig. 2. Correlation amid 25-OH Vit. D and IL-6 (A), 25-OH Vit. D and IL-35 (B), 25-OH Vit. D and IL-10 (C), 25-OH Vit. D and TNF-α (D), 25-OH Vit. D and CRP (E), IL-6 and IL-35 (F), IL-6 and TNF-α (G), IL-6 and IL-10 (H), finally IL-10 and IL-35.
Serum CRP level and correlation with other parameters
Serum CRP level in all patients was 9007 ± 2860. In RA patients 25-OH Vit. D deficient group, CRP level was 9105 ± 2713, but it was 8843 ± 3181in RA patients 25-OH Vit. D sufficient group (Table 2) (Fig. 1), without statistically significant variance between the two groups (P value 0.7828) (Table 2). Interestingly, serum CRP level did not correlate with any parameter present in that study (data not shown).
Table (1):
Baseline characteristics of 25-OH Vit. D for RA patients and healthy volunteers.
Parameter (Mean±SD) |
RA patients |
Healthy volunteers |
P value |
|---|---|---|---|
Vit. D level ng/ml |
16.39 |
22.35 |
0.0193 |
Table (2):
Baseline characteristics of RA patients 25-OH Vit. D deficient and RA patients 25-OH Vit. D sufficient.
Parameter (Mean±SD) |
RA patients with Vit. D deficiency (N=25) |
RA patients with Vit. D sufficiency (N=15) |
P value |
|---|---|---|---|
Age (Years) |
44.12 ± 9.761 |
41.73 ± 7.769 |
0.4258 |
Sex Male: Female |
0 : 25 |
2 : 13 |
|
Vit. D level ng/ml |
12.93 ± 4.753 |
41.40 ± 14.77 |
|
CRP ng/ml |
9105 ± 2713 |
8843 ± 3181 |
0.7828 |
IL-6 ng/L |
5.775 ± 1.822 |
4.539 ± 1.218 |
0.0294 |
TNF-α ng/L |
255.6 ± 50.03 |
250.1 ± 61.01 |
0.7316 |
IL-10 ng/L |
186.1 ± 39.38 |
218.0 ± 42.43 |
0.0234 |
IL-35 pg/ml |
4022 ± 716.3 |
4729 ± 1309 |
0.0356 |
Serum IL-6 cytokine level and correlation with other parameters
IL-6 serum level in all patients was with mean ± SD 5.383 ± 1.731. the serum level of IL-6 in RA patients 25-OH Vit. D deficient group was 5.775 ± 1.822, while in RA patients 25-OH Vit. D sufficient group was 4.539 ± 1.218 (Table 2) (Fig. 1). The variance among the two groups was found to be statistically significant with P value 0.0294. Serum IL-6 level correlated significantly with IL-10 (r = 0.5065, P = 0.0009), IL-35 (r = 0.3829, P = 0.0147) and TNF-a (r = 0.3841, P = 0.0144) (Table 3) (Fig. 2), also, IL-6 level negatively correlated significantly with 25-OH Vit. D. IL-6 did not correlate with CRP (data not shown).
Table (3):
Correlation investigation between parameters present in that study.
Parameter |
IL-6 |
IL-10 |
IL-35 |
TNF-α |
CRP |
|---|---|---|---|---|---|
Vitamin D (25-OH Vit. D) |
r = -0.3188 P = 0.0479 |
r = 0.4516 P = 0.0034 |
r = 0.3424 P = 0.0329 |
r = -0.1141 P = 0.4834 |
r = 0.009931 P = 0.9515 |
IL-10 |
r = 0.5065 P = 0.0009 |
r = 0.6005 P = | |||
IL-6 |
r = 0.3829 P = 0.0147 |
r = 0.3841 P = 0.0144 |
Serum TNF-a level and correlation with other parameters
Serum TNF-a level in all patients was 255.5 ± 58.24. the serum TNF- a in RA patients 25-OH Vit. D deficient group was 255.6 ± 50.03, however it was 250.1 ± 61.01 in RA patients 25-OH Vit. D sufficient group (Table 2) (Fig. 1). Serum TNF- a level variance among the two groups was not statistically significant (P value 0.7316) (Table 2). Furthermore, serum TNF- a level correlated significantly only with serum IL-6 level (Table 3) (Fig. 2), and did not correlate with any other parameter present in that study (25-OH Vit. D, IL-10, IL-35, CRP) (data not shown).
Serum IL-10 cytokine level and correlation with other parameters
Serum IL-10 level in all patients was 196.3 ± 43.05. The serum IL-10 level in RA patients 25-OH Vit. D deficient group was 186.1 ± 39.38, whereas in RA patients 25-OH Vit. D sufficient group was 218.0 ± 42.43 (Table 2) (Fig. 1). The difference in serum IL-10 among the 2 group was statistically significant (P value 0.0234) (Table 2). Serum IL-10 correlated significantly with 25-OH Vit. D serum level (r = 0.4516, P = 0.0034), IL-6 serum level (r = 0.5065, P = 0.0009) and finally with IL-35 serum level (r = 0.6005, P = <0.0001) (Table 2) (Fig. 1). but it did not correlate neither TNF-a nor CRP (data not shown).
Serum IL-35 cytokine level and correlation with other parameters
Serum IL-35 in all patients was 4340 ± 1058. The serum IL-35 in RA patients 25-OH Vit. D deficient group was 4022 ± 716.3, and in RA patients 25-OH Vit. D sufficient group was 4729 ± 1309 (Table 2) (Fig. 1). Moreover, the variance among the 2 groups in IL-35 was statistically significant with P value 0.0356 (Table 2). Serum, IL-35 level correlated significantly with serum 25-OH Vit. D level, serum IL-6 and serum IL-10 (Table 3) (Fig. 2), but in the same time neither TNF-a nor CRP correlated with serum IL-35 level (data not shown).
Many types of inflammatory diseases as RA have been linked to low vitamin D serum level47-50, although many studies reported that serum vitamin D level was not necessary to be lower than in healthy controls49. Our results revealed that, 25 patients having rheumatoid arthritis (RA) (62.5%) were deficient in 25-OH Vitamin D (25-OH Vit. D) level, while only 15 patients with RA (37.5%) were with normal 25-OH Vit. D level. The difference among the RA patients 25-OH Vit. D deficient group (12.93 ± 4.753) and RA patients 25-OH Vit. D sufficient group (41.40 ± 14.77) was statistically significant (P < 0.0001). Many recent studies reported that, decreased serum level of vitamin D is associated with many types of inflammatory diseases as rheumatoid arthritis (RA)47-50. However other studies indicated that, serum level of vitamin D in rheumatic patients is not certainly lower than in healthy volunteers49. A microarray dissection reported that, 5% of the human genome and the physiological attitude of not less than 36 different types of cells are under the regulation of vitamin D either by indirect or direct action51. Furthermore, a recent study reported that, there were no statistically significant variance in vitamin D level between persistent RA or reactive arthritis and healthy control present in that study6, which also support the believe that, vitamin D level is not necessarily correlated with inflammatory disease. Another recent study reported that, 84% of RA patients present in in that study were deficient in serum vitamin D level, while only 34% of healthy control were deficient in serum vitamin D level, not only this, but also vitamin D level were inversely correlated significantly with AR disease activity in that study15. Merlino, Curtis52 reported that, RA risk is noticeably decreased by vitamin D supplement. Furthermore, a recent meta-analysis research revealed that, higher vitamin D deficiency prevalence (55.2%) with significant P value (P = 0.023) in RA patients than in healthy control (33.2%) in 1143 RA patients and 963 healthy controls47. This meta-analysis research also, reported that, the level of vitamin D was inversely correlated with RA disease activity47. In the light of our results and other studies results, we think that, vitamin D deficiency is highly prevailing in RA patients.
TNF- %, IL-17, IL-6 and IL-1 are predominant pro-inflammatory cytokines in RA chronic inflammation of joints by both cartilage and bone distortion53. From recent researches it has been apparent, the value of vitamin D on the health and the activity of many types of diseases, thus beside its well-known role on bone metabolism8,54,55, vitamin D possesses a leading role on the cardiovascular and immune system. It had been approved that, normal vitamin D level is essential for normal physiological function of both innate and adaptive immune response and also for self-antigen tolerance8,56-59. This role is imputed to the ability of vitamin D to increase the expression of the anti-inflammatory cytokines like IL-10 and decrease the expression of pro-inflammatory cytokines such as IL-6 and TNF- a, accordingly vitamin D deficiency is proved to be associated with loss of immune tolerance to self-antigen and thus to autoimmune diseases like RA disease60. In the present study, the serum IL-6 level in all RA patients was 5.383 ± 1.731, moreover, IL-6 was higher in RA patients 25-OH Vit. D deficient group (5.775 ± 1.822) than in RA patients 25-OH Vit. D sufficient group (4.539 ± 1.218) with statistically significant variance (P = 0.0294). In the same time, 25-OH Vit. D level negatively correlated significantly with IL-6 level (r = -0.3188, P = 0.0479). Also, Caraba, Crisan61 revealed that vitamin D had an inverse significant correlation with both IL-6 and TNF-a. An earlier study indicated that, the intensity of systematic inflammation is inversely associated with vitamin D serum level62. Another study reported that, they did not catch any correlation among serum vitamin D level and serum IL-6, moreover they reported that, neither DAS28 score (Score of 28 joints) nor IL-6 differ significantly amid vitamin D diminish and replete groups63. In the light of most previous studies and our result that, IL-6 was higher in RA patients 25-OH Vit. D deficient group (5.775 ± 1.822) than in RA patients 25-OH Vit. D sufficient group (4.539 ± 1.218) with statistically significant difference (P = 0.0294), we support the hypothesis that normal vitamin D level is a vital and has an inhibitory effect on IL-6 cytokine.
TNF promote synovial-fibroblast, endothelial cell and leukocyte activation, pain receptor sensitization and angiogenesis which all together are main characteristics of RA64. Activation of synovial-fibroblast by TNF-a results in the production of CTGF (connective tissue growth factor) causes hyper activation of osteoclasts, leading to joint deterioration65. In our study, the serum TNF-a in all patients was 255.5 ± 58.24. Furthermore, in RA patients 25-OH Vit. D deficient group TNF-a serum level was 255.6 ± 50.03 and in RA patients 25-OH Vit. D sufficient group was 250.1 ± 61.01 without significant variance (P = 0.7316) amid the two groups. Likewise, 25-OH Vit. D level did not correlate with TNF-a level (r = -0.1141, P = 0.4834) and this is in agreement with previous study66. Another study reported that, there were no significant variance in serum TNF-a level amid vitamin D sufficiency group and vitamin D deficiency group67. Also they reported that, increased sTNFr1 (soluble tumor necrosis factor-receptor-1) and decreased sTNFr2 (soluble tumor necrosis factor-receptor-2) significantly in vitamin D sufficiency group than in vitamin D deficiency group67. Thus, based on the results of our study and the mentioned previous studies, serum TNF-a is not affected by serum vitamin D status without vitamin D supplement.
Our study revealed that, the serum CRP in all patients was 9007 ± 2860. The CRP level in RA patients 25-OH Vit. D deficient group was 9105 ± 2713, and in RA patients 25-OH Vit. D sufficient group was 8843 ± 3181 without statistically significant variance amid the two groups (P = 0.7828). Also, serum vitamin D level did not correlate with serum CRP level (r = 0.009931, P = 0.9515). These findings agree with previous study (63). The pro-inflammatory cytokine IL-6 is linked with CRP release68, thus, based on this finding and our results, we believe that, vitamin D status without supplement has no effect on neither IL-6 nor its role in releasing acute phase proteins.
Our study revealed that, serum level of IL-35 in all patients was 4340 ± 1058. Interestingly, IL-35 was higher in RA patients 25-OH Vit. D sufficient group (4729 ± 1309) than RA patients 25-OH Vit. D deficient group (4022 ± 716.3) with significant difference (P = 0.0356). Furthermore, serum 25-OH Vit. D level correlated significantly with serum IL-35 (r = 0.3424, P = 0.0329). the data about IL-35 is controversial, that early study reported that an early study reported that, in-vitro TNF a stimulation resulted in enhancing the expression of both p35 and EBI3 subunits of IL-3569. Not only this but also IL-35 itself stimulated the expression of many pro-inflammatory particles in mononuclear cells69. In collagen induced arthritis (CIA) mice model, IL-35 was used as remedy for CIA mice orally by using the engineered Lactococcus lactis strain as vector70. IL-35 exhibited anti-inflammatory properties by significantly decreasing IFN-γ and IL-17 levels and increasing the level of both IL-10 and CCR6+ Tregs (regulatory T cells)70, thus, this supporting the anti-inflammatory features of IL-35. Another study reported that, IL-35 possesses a role in Treg-mediated repression of autoimmunity in RA71. Another studies confirmed the role of IL-35 in hindering the processes linked to (vascular endothelial growth factor) VEGF/Ang2/Tie2 pathway72,73, also they indicated that IL-35 activity stimulated neovascularization, and promoted inflammatory process during the acute phase of RA72. Moreover,74 reported that IL-35 is positively correlated significantly with Treg percentage, and in the same time Trge percentage negatively correlated with DAS28 in RA patients, which confirm the anti-inflammatory effect of IL-35 in RA.
Interestingly, in the current study, IL-35 also, correlated significantly with both IL-6 (r = 0.3829, P = 0.0147) and IL-10 (r = 0.6005, P = <0.0001). The immunomodulatory effect of IL-35 as anti-inflammatory may be due to its ability to upregulate the expansion of both regulatory T cells and IL-10 and in the same time inhibit the differentiation of Th 17 cells and suppress the proliferation of Teff cells39,42. However, another study reported that, IL-35 inversely correlated significantly with 28-joint DAS and in the same time in contrast to our results, IL-35 did not correlate with IL-1071. Furthermore, another study reported that, Tregs are divided into two distinct subsets; one subsets produce the suppressive cytokine IL-35 and CCR7, located in the T cell zone, while the other subset producing high level of the suppressive cytokine IL-10,granzymes, ICOS and multiple chemokine receptors responsible for migration to peripheral non-lymphoid tissues75.
Also, we found that IL-6 correlated significantly with IL-10 (r = 0.5065, P = 0.0009). it was reported that; higher level of IL-10 is produced in response to higher inflammatory state in patients with RA66.
Finally, our results revealed that, IL-6 correlated significantly with TNF-a (r = 0.3841, P = 0.0144) which is in agreement with other studies (76). It was reported that inhibition of TNF- a in a synovial cell culture resulted in down regulation of the production of other pro-inflammatory cytokines77. It was reported that TNF-a promote the production of IL-6 from synoviocytes in RA patients78.
This study demonstrated that, serum level of IL-10 and IL-35 were higher in 25-OH Vit. D sufficient group than 25-OH Vit. D deficient group with significant difference. also IL-6 serum level was lower in in 25-OH Vit. D sufficient group than 25-OH Vit. D deficient group with significant difference. the levels of TNF-a and CRP also were lower in 25-OH Vit. D sufficient group than 25-OH Vit. D deficient group without significant difference. also 25-OH Vit. D correlated significantly with both IL-10 and IL-35, and in the same time 25-OH Vit. D negatively correlated significantly with IL-6. From our study the sufficient 25-OH Vit. D serum level could potentiate the production of anti-inflammatory cytokines (IL-10 and IL-35) and also could repress the release of pro-inflammatory IL-6. Thus we support the hypothesis that 25-OH Vit. D act as immunomodulatory agent in RA diseases and the serum level of 25-OH Vit. D is important and must be assessed for all patients with not only RA disease but also for all inflammatory autoimmune diseases.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors designed the experiments. R performed the experiments. H and M analyzed the data. S and S wrote the manuscript. All authors read and approved the manuscript.
FUNDING
This study was supported by 50% of the cost from Deraya University. Grant number is 2852019-1:56.
ETHICS STATEMENT
That study was conducted during 2019 after approval of the ethical committee of the university hospital (Ref number 17100135). A written informed consent was obtained after discussing a detailed description of the study with the patient. Patients were informed that they can withdraw their consent to participate at any time. The work was done in agreement with the Declaration of Helsinki.
AVAILABILITY OF DATA
All datasets generated or analyzed during this study are included in the manuscript.
- Malmstrom V, Catrina AI, Klareskog L. The immunopathogenesis of seropositive rheumatoid arthritis: from triggering to targeting. Nat Rev Immunol. 2017;17(1):60-75.
Crossref - Holick MF. Resurrection of vitamin D deficiency and rickets. J Clin Invest. 2006;116(8):2062-2072.
Crossref - Brunette MG, Chan M, Ferriere C, Roberts KD. Site of 1, 25 (OH)2 vitamin D3 synthesis in the kidney. Nature. 1978;276:287-289.
Crossref - Shils ME, Shike M. Modern nutrition in health and disease: Lippincott Williams & Wilkins. 2006.
- Norman A. In Present Knowledge in Nutrition, eds EE Ziegler and LJ Filer, Jr. ILSI Press, Washington, DC. 1996.
- Li D, Jeffery LE, Jenkinson C, et al. Serum and synovial fluid vitamin D metabolites and rheumatoid arthritis. J Steroid Biochem Mol Biol. 2019;187:1-8.
Crossref - Cantorna MT, Zhu Y, Froicu M, Wittke A. Vitamin D status, 1, 25-dihydroxyvitamin D3, and the immune system. Am J Clin Nutr. 2004;80(6 suppl):1717S-1720S.
Crossref - Deluca HF, Cantorna MT. Vitamin D: its role and uses in immunology. The FASEB Journal. 2001;15(14):2579-2585.
Crossref - Tetlow LC, Smith SJ, Mawer EB, Woolley DE. Vitamin D receptors in the rheumatoid lesion: expression by chondrocytes, macrophages, and synoviocytes. Ann Rheum Dis. 1999;58(2):118-121.
Crossref - Cantorna M, Hayes C, DeLuca H. 1, 25-dihydroxyvitamin D3 prevents and ameliorates symptoms in two experimental models of human arthritis. J Allergy Clin Immunol. 1997;99(1).
- Jones BJ, Twomey PJ. Issues with vitamin D in routine clinical practice. Rheumatology (Oxford). 2008;47(9):1267-1268.
Crossref - Cantorna MT. Vitamin D and Autoimmunity: Is Vitamin D Status an Environmental Factor Affecting Autoimmune Disease Prevalence?. Proceedings of the Society for Experimental Biology and Medicine. 2000;223(3):230-233.
Crossref - Kamen DL, Cooper GS, Bouali H, Shaftman SR, Hollis BW, Gilkeson GS. Vitamin D deficiency in systemic lupus erythematosus. Autoimmunity Reviews.2006;5(2):114-117.
Crossref - Lips P. Which circulating level of 25-hydroxyvitamin D is appropriate? J Steroid Biochem Mol Biol. 2004;89:611-614.
Crossref - Meena N, Chawla SPS, Garg R, Batta A, Kaur S. Assessment of vitamin D in rheumatoid arthritis and its correlation with disease activity. J Nat Sci Biol Med. 2018;9(1):54-58.
Crossref - Candido FG, Bressan J. Vitamin D: link between osteoporosis, obesity, and diabetes? Int J Mol Sci. 2014;15(4):6569-6591.
Crossref - Mosaad YM, Hammad EM, Fawzy Z, et al. Vitamin D receptor gene polymorphism as possible risk factor in rheumatoid arthritis and rheumatoid related osteoporosis. Hum Immunol. 2014;75(5):452-461.
Crossref - Hussien YM, Shehata A, Karam RA, Alzahrani SS, Magdy H, El-Shafey AM. Polymorphism in vitamin D receptor and osteoprotegerin genes in Egyptian rheumatoid arthritis patients with and without osteoporosis. Mol Biol Rep. 2013;40(5):3675-3680.
Crossref - Tizaoui K, Kaabachi W, Salah MO, Amor AB, Hamzaoui A, Hamzaoui K. Vitamin D receptor TaqI and ApaI polymorphisms: a comparative study in patients with Behcet’s disease and Rheumatoid arthritis in Tunisian population. Cell Immunol. 2014;290(1):66-71.
Crossref - Tizaoui K, Hamzaoui K. Association between VDR polymorphisms and rheumatoid arthritis disease: systematic review and updated meta-analysis of case-control studies. Immunobiology. 2015;220(6):807-816.
Crossref - Ritterhouse LL, Crowe SR, Niewold TB, et al. Vitamin D deficiency is associated with an increased autoimmune response in healthy individuals and in patients with systemic lupus erythematosus. Ann Rheum Dis. 2011;70(9):1569-1574.
Crossref - Ranganathan P. Genetics of bone loss in rheumatoid arthritis-role of vitamin D receptor polymorphisms. Rheumatology. 2009;48(4):342-346.
Crossref - Muller K, Bendtzen K. Inhibition of human T lymphocyte proliferation and cytokine production by 1, 25-dihydroxyvitamin D3. Differential effects on CD45RA+ and CD45R0+ cells. Autoimmunity. 1993;14(1):37-43.
Crossref - Simsek I. TNF inhibitors for rheumatoid arthritis. Bulletin of the NYU Hospital for Joint Diseases. 2011;69(3):220-224.
- Brand DD, Latham KA, Rosloniec EF. Collagen-induced arthritis. Nat Protoc. 2007;2(5):1269-1275.
Crossref - Suematsu S, Matsuda T, Aozasa K, et al. IgG1 plasmacytosis in interleukin 6 transgenic mice. Proc Natl Acad Sci USA. 1989;86(19):7547-7551.
Crossref - Suzuki M, Hashizume M, Yoshida H, Shiina M, Mihara M. IL-6 and IL-1 synergistically enhanced the production of MMPs from synovial cells by up-regulating IL-6 production and IL-1 receptor I expression. Cytokine. 2010;51(2):178-183.
Crossref - Van Snick J. Interleukin-6: an overview. Annual Review of Immunology. 1990;8(1):253-278.
Crossref - Zhang Y, Leung DY, Richers BN, et al. Vitamin D inhibits monocyte/macrophage proinflammatory cytokine production by targeting MAPK phosphatase-1. The Journal of Immunology. 2012;188(5):2127-2135.
Crossref - Nonn L, Peng L, Feldman D, Peehl DM. Inhibition of p38 by vitamin D reduces interleukin-6 production in normal prostate cells via mitogen-activated protein kinase phosphatase 5: implications for prostate cancer prevention by vitamin D. Cancer Research. 2006;66(8):4516-4524.
Crossref - Correale J, Ysrraelit MC, Gaitan MI. Immunomodulatory effects of Vitamin D in multiple sclerosis. Brain. 2009;132(5):1146-1160.
Crossref - Cantorna MT, Hayes CE, DeLuca HF. 1, 25-Dihydroxycholecalciferol inhibits the progression of arthritis in murine models of human arthritis. J Nutr. 1998;128(1):68-72.
Crossref - Boonstra A, Barrat FJ, Crain C, Heath VL, Savelkoul HF, O’Garra A. 1a, 25-Dihydroxyvitamin D3 has a direct effect on naive CD4+ T cells to enhance the development of Th2 cells. The Journal of Immunology. 2001;167(9):4974-4980.
Crossref - Cush JJ, Splawski JB, Thomas R, et al. Elevated interleukin-10 levels in patients with rheumatoid arthritis. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology. 1995;38(1):96-104.
Crossref - Bober LA, Rojas-Triana A, Jackson JV, et al. Regulatory effects of interleukin-4 and interleukin-10 on human neutrophil function ex vivo and on neutrophil influx in a rat model of arthritis. Arthritis & Rheumatism. 2000;43(12):2660-2667.
Crossref - Smallie T, Ricchetti G, Horwood NJ, Feldmann M, Clark AR, Williams LM. IL-10 inhibits transcription elongation of the human TNF gene in primary macrophages. Int J Clin Exp Med. 2010;207(10):2081-2088.
Crossref - Choi J, Leung PS, Bowlus C, Gershwin ME. IL-35 and autoimmunity: a comprehensive perspective. Clin Rev Allergy Immunol. 2015;49(3):327-332.
Crossref - Collison LW, Delgoffe GM, Guy CS, et al. The composition and signaling of the IL-35 receptor are unconventional. Nat immunol. 2012;13(3):290-299.
Crossref - Collison LW, Workman CJ, Kuo TT, et al. The inhibitory cytokine IL-35 contributes to regulatory T-cell function. Nature. 2007;450(7169):566-569.
Crossref - Shen P, Roch T, Lampropoulou V, et al. IL-35-producing B cells are critical regulators of immunity during autoimmune and infectious diseases. Nature. 2014;507(7492):366-370.
Crossref - Wang R-X, Yu C-R, Dambuza IM, et al. Interleukin-35 induces regulatory B cells that suppress autoimmune disease. Nat Med. 2014;20(6):633-641.
Crossref - Niedbala W, Wei Xq, Cai B, et al. IL-35 is a novel cytokine with therapeutic effects against collagen-induced arthritis through the expansion of regulatory T cells and suppression of Th17 cells. Eur J Immunol. 2007;37(11):3021-3029.
Crossref - Li Y, Wu S, Li Y, et al. Interleukin-35 (IL-35) inhibits proliferation and promotes apoptosis of fibroblast-like synoviocytes isolated from mice with collagen-induced arthritis. Mol Biol Rep. 2016;43(9):947-956.
Crossref - Wu S, Li Y, Li Y, et al. Interleukin-35 attenuates collagen-induced arthritis through suppression of vascular endothelial growth factor and its receptors. Int Immunopharmacol. 2016;34:71-77.
Crossref - Aletaha D, Neogi T, Silman AJ, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann Rheum Dis. 2010;69(9):1580-1588.
Crossref - Aletaha D, Ward MM, Machold KP, Nell VP, Stamm T, Smolen JS. Remission and active disease in rheumatoid arthritis: defining criteria for disease activity states. Arthritis and Rheumatism. 2005;52(9):2625-2636.
Crossref - Lee YH, Bae SC. Vitamin D level in rheumatoid arthritis and its correlation with the disease activity: a meta-analysis. Clin Exp Rheumatol. 2016;34(5):827-33.
- Lin J, Liu J, Davies ML, Chen W. Serum vitamin D level and rheumatoid arthritis disease activity: review and meta-analysis. PloS one. 2016;11(1):e0146351.
Crossref - Cecchetti S, Tatar Z, Galan P, Pereira B, Lambert C, Mouterde G, et al. Prevalence of vitamin D deficiency in rheumatoid arthritis and association with disease activity and cardiovascular risk factors: data from the COMEDRA study. Clin Exp Rheumatol. 2016;34(6):984-90.
- Vojinovic J, Tincani A, Sulli A, et al. European multicentre pilot survey to assess vitamin D status in rheumatoid arthritis patients and early development of a new Patient Reported Outcome questionnaire (D-PRO). Autoimmunity Reviews. 2017;16(5):548-554.
Crossref - Hossein-nezhad A, Holick MF, editors. Vitamin D for health: a global perspective. Mayo Clinic Proceedings, Elsevier. 2013;88(7);720-755.
Crossref - Merlino LA, Curtis J, Mikuls TR, Cerhan JR, Criswell LA, Saag KG. Vitamin D intake is inversely associated with rheumatoid arthritis: results from the Iowa Women’s Health Study. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology. 2004;50(1):72-77.
Crossref - Georgopoulos S, Plows D, Kollias G. Transmembrane TNF is sufficient to induce localized tissue toxicity and chronic inflammatory arthritis in transgenic mice. Journal of inflammation. 1996;46(2):86-97.
- Melamed ML, Michos ED, Post W, Astor B. 25-hydroxyvitamin D levels and the risk of mortality in the general population. Arch Intern Med. 2008;168(15):1629-1637.
Crossref - Kim DH, Sabour S, Sagar UN, Adams S, Whellan DJ. Prevalence of hypovitaminosis D in cardiovascular diseases (from the National Health and Nutrition Examination Survey 2001 to 2004). Am J Cardiol. 2008;102(11):1540-1544.
Crossref - Hong Q, Xu J, Xu S, Lian L, Zhang M, Ding C. Associations between serum 25-hydroxyvitamin D and disease activity, inflammatory cytokines and bone loss in patients with rheumatoid arthritis. Rheumatology. 2014;53(11):1994-2001.
- Maruotti N, Cantatore FP. Vitamin D and the immune system. J Rheumatol. 2010;37(3):491-495.
Crossref - Hewison M. An update on vitamin D and human immunity. Clinical Endocrinology. 2012;76(3):315-325.
Crossref - Lequerre T, Richez C. Pathophysiology of rheumatoid arthritis. La Revue du Praticien. 2012;62(8):1085-1093.
- Zittermann A, Schleithoff SS, Koerfer R. Putting cardiovascular disease and vitamin D insufficiency into perspective. Br J Nutr. 2005;94(4):483-492.
Crossref - Caraba A, Crisan V, Romosan I, Mozos I, Murariu M. Vitamin D status, disease activity, and endothelial dysfunction in early rheumatoid arthritis patients. Disease Markers. 2017;2017.
Crossref - Welsh P, Peters MJ, Sattar N. Is vitamin D in rheumatoid arthritis a magic bullet or a mirage? The need to improve the evidence base prior to calls for supplementation. Arthritis & Rheumatism. 2011;63(7):1763-1769.
Crossref - Gopal K, Thevarajah M, Ng CM, Raja J. Effects of vitamin D on disease activity and serum interleukin-6 in rheumatoid arthritis. Int J Rheum Dis. 2019;22(5):834-841.
Crossref - McInnes IB, Schett G. Cytokines in the pathogenesis of rheumatoid arthritis. Nat Rev Immunol. 2007;7(6):429-442.
Crossref - Nozawa K, Fujishiro M, Takasaki Y, Sekigawa I. Inhibition of rheumatoid arthritis by blocking connective tissue growth factor. World J Orthop. 2014;5(5):653-659.
Crossref - Mateen S, Moin S, Shahzad S, Khan AQ. Level of inflammatory cytokines in rheumatoid arthritis patients: Correlation with 25-hydroxy vitamin D and reactive oxygen species. PloS one. 2017;12(6):e0178879.
Crossref - Tyler B, Kimberly BB, Victoria ER. Soluble TNF Receptors are Modulated by Vitamin D Status but not by Acute Perturbations in 25-Hydroxyvitamin D Following A Bolus of Supplemental Vitamin D. Journal of Cytokine Biology. 2017;2(2):118.
- Yoshida Y, Tanaka T. Interleukin 6 and rheumatoid arthritis. BioMed Research International. 2014;2014.
Crossref - Filkova M, Vernerova Z, Hulejova H, Prajzlerova K, Veigl D, Pavelka K, et al. Pro-inflammatory effects of interleukin-35 in rheumatoid arthritis. Cytokine. 2015;73(1):36-43.
Crossref - Maddaloni M, Kochetkova I, Hoffman C, Pascual D. Delivery of IL-35 by Lactococcus lactis Ameliorates Collagen-Induced Arthritis in Mice. Front Immunol. 2018;9:2691.
Crossref - Nakano S, Morimoto S, Suzuki S, Tsushima H, Yamanaka K, Sekigawa I, et al. Immunoregulatory role of IL-35 in T cells of patients with rheumatoid arthritis. Rheumatology. 2015;54(8):1498-1506.
Crossref - Wojdasiewicz P, Wajda A, Haladyj E, Romanowska-Prochnicka K, Felis-Giemza A, Nalecz-Janik J, et al. IL-35, TNF-a, BAFF, and VEGF serum levels in patients with different rheumatic diseases. Reumatologia. 2019;57(3):145-150.
Crossref - Jiang S, Li Y, Lin T, Yuan L, Li Y, Wu S, et al. IL-35 inhibits angiogenesis through VEGF/Ang2/Tie2 pathway in rheumatoid arthritis. Cell Physiol Biochem. 2016;40(5):1105-1116.
Crossref - Zhang X, Zhang X, Zhuang L, Xu C, Li T, Zhang G, et al. Decreased regulatory Tcell frequency and interleukin35 levels in patients with rheumatoid arthritis. Exp Ther Med. 2018;16(6):5366-5372.
Crossref - Wei X, Zhang J, Gu Q, Huang M, Zhang W, Guo J, et al. Reciprocal expression of IL-35 and IL-10 defines two distinct effector Treg subsets that are required for maintenance of immune tolerance. Cell Reports. 2017;21(7):1853-1869.
Crossref - Manicourt DH, Triki R, Fukuda K, Devogelaer JP, Deuxchaisnes CND, Thonar EJM. Levels of circulating tumor necrosis factor a and interleukin-6 in patients with rheumatoid arthritis. relationship to serum levels of hyaluronan and antigenic keratan sulfate. Arthritis & Rheumatism: Official Journal of the American College of Rheumatology. 1993;36(4):490-499.
Crossref - Mateen S, Zafar A, Moin S, Khan AQ, Zubair S. Understanding the role of cytokines in the pathogenesis of rheumatoid arthritis. Clinica Chimica Acta. 2016;455:161-171.
Crossref - Lee A, Qiao Y, Grigoriev G, Chen J, Park-Min KH, Park SH, et al. Tumor necrosis factor a induces sustained signaling and a prolonged and unremitting inflammatory response in rheumatoid arthritis synovial fibroblasts. Arthritis & Rheumatism. 2013;65(4):928-938.
Crossref
© The Author(s) 2020. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.