

ISSN: 0973-7510
E-ISSN: 2581-690X
Evidence concerning prescription audits conducted in developing countries like India is scarce, especially from the rural parts of the country. Therefore, the present prescription audit was undertaken in a rural tertiary care hospital to investigate prescriptions for their completeness, in format of prescription, legibility of writing and it was assessed against the World Health Organization (WHO) recommendation of core indicators for prescription writing in order to investigate the rational usage of drugs. A total of 200 prescriptions were randomly selected, irrespective of clinical departments, patient characteristics and diagnosis over a period of six months. All the prescriptions were prospectively analyzed and conferred to an assessment of the quality of prescribing practice, general details, medical components, WHO core drug use indicators and legibility. Amongst the 200 prescriptions precisely monitored, we found that 100% prescriptions had general details of the patients such as name, age, gender, OPD/IPD registration number, hospital name & address and consulting unit/department. While evaluating the handwriting of the doctors, 83.5% (177/200) of the prescriptions had legible handwriting, wherein the degree of legibility showed 68.5% (137/200) prescriptions with easy legibility, 20% (40/200) difficult legibility while 11.5% (23/200) were illegible. Along with the different types of drugs obtained from the selected prescriptions, we found that antibiotics were prescribed in 51.5% (103/200) of the prescriptions. A prescription audit is a good tool to systemically review the day to day work, maintenance of records and assessment of accuracy of the diagnosis given by doctors and also the outcome of the treatment received.
Prescription audit, tertiary care hospital, legibility, antibiotics
A prescription audit (PA) is a systematic and critical analysis of the quality of prescribed medical care, which includes procedures used for diagnostic and treatment purposes, the appropriate use of various resources, and the resulting outcome on the quality of life of patients. It is an active process that checks for improvement in quality of health care.1 Being a continuous cycle in nature, PA involves observing various practices followed, setting standards for comparison, comparing followed practices with set standards, implementing changes as required and observing for new practices.1 A PA is defined as “the review and evaluation of health-care procedures and their documentation to compare the quality of care which are being provided, with the accepted set standards”.2-4 Prescription writing assessment is considered an important parameter to ensure rational drug use.5 Rational use of drugs is essential to achieve good quality health care for patients as well as for the community.5 It ensures that patients are advised medications which are appropriate for their clinical needs and in doses that suits each patient’s individual requirements and that they are prescribed for adequate period with minimum cost to patients and the community.6 Irrational prescription may lead to ineffective treatment, which may subject the patient to prolongation or exacerbation of illness, unnecessary mental distress, untoward side effects and higher expenses.7 The World Health Organization (WHO) formulates a set of “core prescribing indicators” which aims at improvement of rational drug use for outpatient practices. It includes indicators for prescription, indicators for patient care and also indicators for various facilities.8 Based on such indicators, various studies have been done in countries across the globe, including India.1,2,4,5,8 With the use of such prescribing indicators, auditing prescription forms is an important part of drug utilization studies. These include, but are not limited to average time for consultation, average time for dispensing of medicines/ drugs, actual percentage of dispensed drugs, percentage of drugs labelled correctly, knowledge of patients regarding correct drug dosage and also facility indicators which include availability of key drugs and an essential drug formulary.9
An ideal prescription should include the full name of patient, age, address, hospital registration number of the patient, date of prescription, the clinical diagnosis and clearly specify the generic name of the drug being used, formulation used with the dose, frequency of administration and total quantity of the drug to be supplied for the duration of the treatment. This should be completed by signature of the prescribing physician indicating one’s name, medical registration number and if possible one’s address.10 The assessment of prescribing patterns should aim to monitor and evaluate current prescription practices and suggest appropriate modifications as required in prescribing practices followed by medical practitioners for rationalizing medical care and make it more cost-effective.11 Additionally, as a large amount of resources are spent on drugs, regular monitoring of drug prescriptions are essential and drug administration and formulate appropriate measures to correct the errors detected so as to ensure effective utilization of the resources spent.11
The hospital chosen for the present prescription audit is a rural tertiary care hospital which meets the health needs of the majority of rural and peri-urban populations in and around Gurugram. Since regular prescription auditing has never been undertaken at this hospital, the present study served as a tool to evaluate the prescribing practices of the physicians in an attempt to optimize and investigate the rational use of drugs by evaluating the completeness of the prescription written, legibility of handwriting of the prescribing physician and assess the parameters against the core indicators for drug use recommended by the WHO.
Study setting and study population
The present study is a prospective, observational hospital-based study that was carried out between January 2020 to June 2020 at SGT Hospital, Gurugram, Haryana, India. A total of 200 prescriptions from patient of both the sexes of any age group attending both OPD and IPD departments during the period of study were randomly selected. Those patients attending OPD for Tetanus Toxoid (TT) and other vaccines and neonates (≤ 28 days) were excluded from the study. The protocol of the study was approved by the institutional ethics committee of SGT University. Complete confidentiality of patients was maintained throughout the research process and informed written consent was obtained at initiation.
Data collection
The patients receiving medications during their treatment visits were documented and 200 prescriptions were randomly selected, irrespective of characteristics of patient, their diagnosis and the clinical department.
Source of data
Prescription copies were collected from the various departments, after taking prior permission from the hospital authority, data were stored, documented and the data scrutiny procedures were adopted as well as were reported to the quality department for further analysis. The prescriptions reaching the quality department were analyzed for patient information (patient initials, patient’s sex and age), general information (patient IP number) and prescribed drug information drug allergy, route of administration, drug strength, frequency of dose, indication/diagnosis, 1, 2 and >2 antibiotics, date, signature of the clinician, therapeutic duplication/ alternate drug, drug written in capital letters, drugs prescribed by generic or brand names and legibility of prescriptions.
The WHO core indicators for drug use which include three groups were precisely monitored in the selected prescriptions viz. a) prescribing indicators: percentage of drugs prescribed by their generic name, average number of drugs per prescription, percentage of prescriptions containing antimicrobial agents, percentage of injections per prescription and percentage of drugs prescribed from the Essential Drug List (EDL), b) patient-care indicators: average time for consultation, dispensing actual percentage of drugs dispensed, percentage of adequate adequately labeled and knowledge of patients on correct dosage and c) indicators of health facility: availability of EDL copy in all OPDs and IPDs and availability of key drugs.12
Data analysis
All the data obtained during the study were entered in Microsoft Excel, expressed as a percentage and analyzed by descriptive statistics. Furthermore, the collected data were analyzed using SPSS version 2020.20
Department wise distribution of prescriptions
A total of 200 prescriptions were obtained from 10 different departments including General medicine (15.5%, n= 31), General surgery (13.5%, n= 27), ENT (10.5%, n= 21), Obstetrics and Gynaecology (13%, n= 26), Ophthalmology (3.5%, n= 07), Psychiatry (1.5%, n= 03), Dermatology (11.5%, n= 23), Paediatrics (9%, n= 18), Orthopaedics (12%, n= 24) and Pulmonary medicine (10%, n= 20) (Table 1). The average waiting time according to our study was found to be 10.03 min/patient (not given in the table).
Table (1):
Department wise distribution of prescriptions included in the study.
No |
Departments |
Number of prescriptions, n (%) |
|---|---|---|
1 |
General Medicine |
31 (15.5) |
2 |
General Surgery |
27 (13.5) |
3 |
Obstetrics & Gynaecology |
26 (13) |
4 |
Orthopaedics |
24 (12) |
5 |
ENT |
21 (10.5) |
6 |
Pulmonary Medicine |
20 (10) |
7 |
Dermatology |
23 (11.5) |
8 |
Ophthalmology |
07 (3.5) |
9 |
Paediatrics |
18 (9) |
10 |
Psychiatry |
03 (1.5) |
TOTAL |
200 (100) |
Evaluation of various prescription parameters
Amongst the 200 prescriptions precisely monitored, we found that all 200 prescriptions (100%) had general details of the patients such as name, age, gender, OPD/IPD registration number as well as identity of the concerned department (Table 2). The age group of the patients ranged from 8 months to 52 years (mean age 30.3±12.5 years) and most of them were males, with male:female ratio as 1:1.1. The name of the visiting units and hospital address were printed on 100% of the prescriptions and 95.5% (191/200) of the prescriptions had the patient’s address printed (Table 2). The consulting doctor’s initials were observed in only 12% (24/200) of the prescriptions instead of full name and signature. Of the prescriptions selected, 13.5% (27/200) mentioned the weight of the patient (Table 2), of which 66.7% (18/27) were children (≤ 1 year of age) and the remaining 33.3% (9/27) were adults. The consultation date was mentioned on 97.5% (195/200) of the prescriptions. Furthermore, 83.5% (177/200) of the prescriptions had legible handwriting, wherein the degree of legibility showed 68.5% (137/200) prescriptions with easy legibility, 20% (40/200) difficult legibility and finally 11.5% (23/200) were illegible (Fig. 1). Regarding medical interventions, surprisingly, we found that only 29.5% (59/200) of the prescriptions had a presumptive or definitive diagnosis mentioned (Table 2).
Table (2):
Evaluation of various prescription parameters audited.
Details |
Prescription frequency, n (%) |
|---|---|
Hospital Name & Address |
200 (100) |
Date of Visit |
195 (97.5) |
Consulting Unit/Department |
200 (100) |
Patient Name |
200 (100) |
Patient Address |
191 (95.5) |
Patient Age & Sex |
200 (100) |
Patient Weight |
27 (13.5) |
Clinician’s Initials |
24 (12) |
Diagnosis |
59 (29.5) |
Generic Name |
137 (68.5) |
EDL of hospital |
200 (100) |
Start Dose Date |
197 (98.6) |
Drug Strength |
54 (27.1) |
Duration of drug intake |
100 (50) |
Route of drug administration |
123 (61.5) |
Over dosing or Under dosing |
0 |
Follow up advice |
62 (31) |
Allergy Status |
0 |
Prescribed Antibiotics |
103 (51.5) |
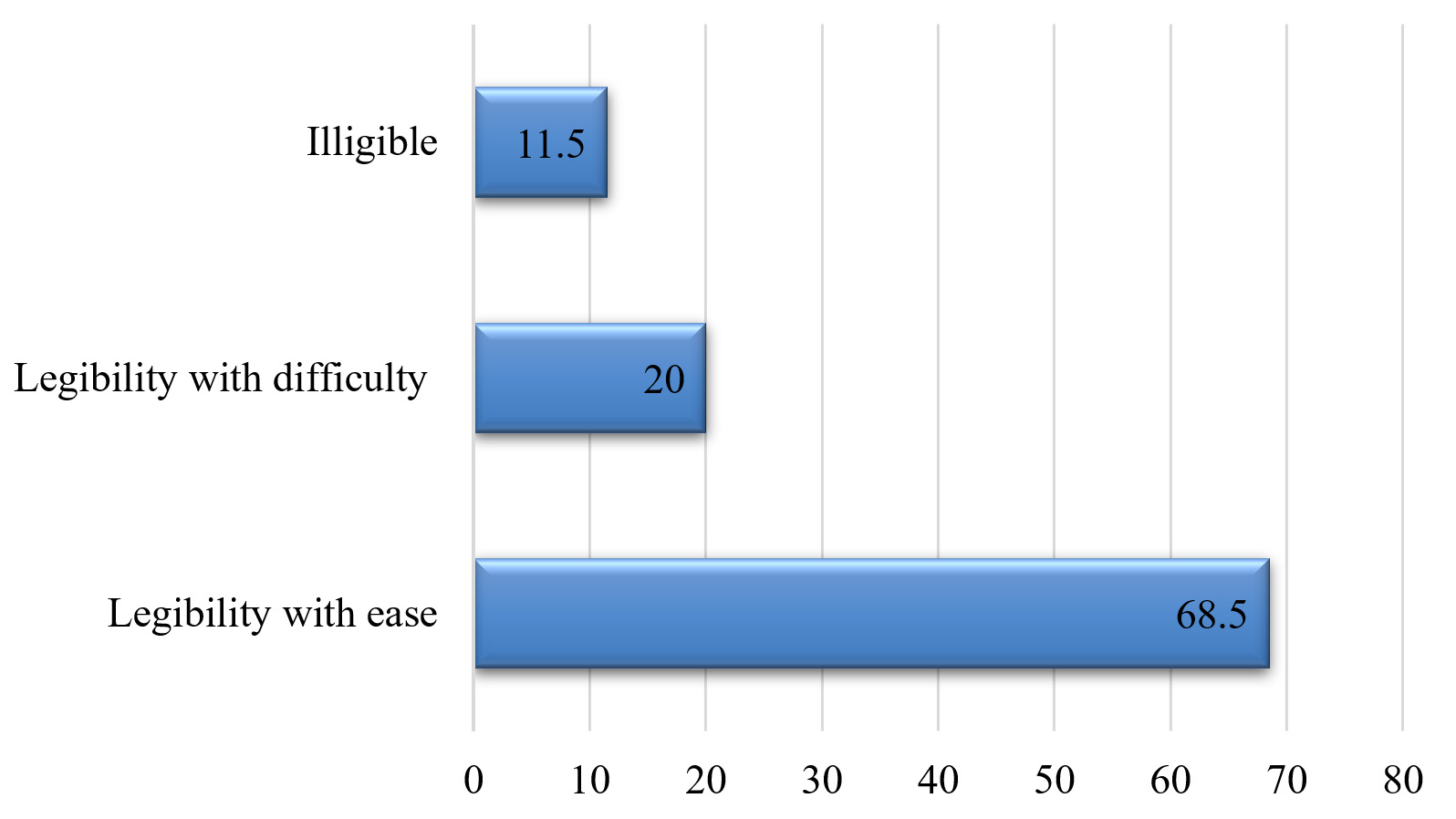
Fig. 1. Percentage of degree of legibility in the prescription.
Data on the WHO core prescribing indicators were analyzed. It was observed that the average number of drugs prescribed was found to be 3.4±0.8. A total of 68.5% (137/200) of the drugs were prescribed by their generic name whereas 28% (56/200) of the drugs were prescribed from EDL of the hospital. None of the prescriptions mentioned the allergy status of the patient (Table 2). Drug dose start date was mentioned in 98.6% (197/200) of the prescriptions whereas the duration of drug intake was mentioned among 50% (100/200) of the prescriptions. Strength of prescribed drug were mentioned in 27.14% (54/200) of the selected prescriptions (Table 2). It was observed in the study that only 35% (70/200) prescriptions had a written instruction on the duration of drug treatment and about 61.5% (123/200) on the route of administration of which oral route was the most common route (88.6%, 109/123) followed by intravenous 5.7% (7/123) and other routes (5.7%, 7/123). Of the total no. of intravenous routes (excluding vaccines) (n= 7), the percentage of injections per prescription was found to be 3.2%. None of the prescriptions stated anything related to the under dosing or overdosing related to prescribed drugs. Follow up advice was clearly mentioned in 31% (62/200) prescriptions obtained from various units (Table 2).
While evaluating the data on the WHO core patient-care indicators, the average consultation time was found to be 7.3±0.6 mins while drug dispensing time on average was 4.4±0.7 minutes. The percentage of drug actually dispensed was found to be 88% (176/200) and all the drugs were adequately labelled. The patients were asked to repeat the instructions received for taking the drugs and it was found that 46% (96/200) of the patients had knowledge of correct drug dosage.
The WHO core health facility indicators were analyzed and it was found that in all the OPDs the copy of EDL was available. About 90% (180/200) of the key drugs were available in the pharmacy of the hospital.
Antibiotic prescription pattern
Along with the different types of drugs obtained from the selected prescriptions, we found that antibiotics were prescribed in 51.5% (103/200) of the prescriptions wherein only one antibiotic was mentioned amongst 40% (80/200) of the medicine cards and a combination of two antibiotics was mentioned in 11.5% (23/200) of the prescription. None of the prescriptions contained more than two antibiotics for any of the patients (Fig. 2).
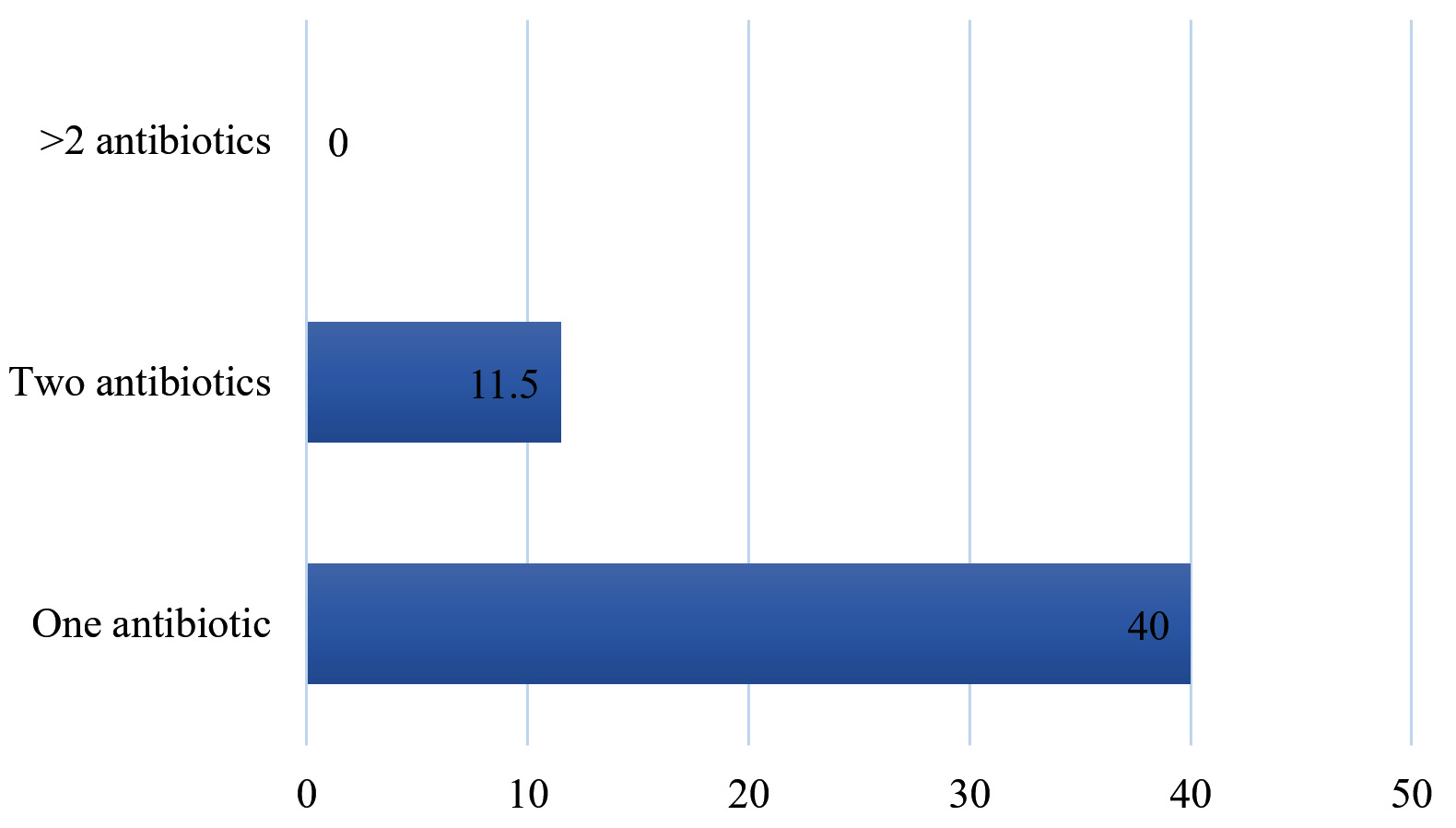
Fig. 2. Percentage wise pattern of antibiotics prescribed
One of the most essential aspects of an optimally functioning healthcare system is judged by its ability to deliver the right medicine to the right patient. Prescriptions are an important intervention for the physician and it is an ethical and legal duty on behalf of the practitioner to write complete prescriptions with generic drug names in legible hand writing.5 Prescription auditing is used as one of the important tools to assess misuse of drugs as well to improve the rational usage of drugs.5
Keeping this in mind, the present study was undertaken by quality assessing committee members of SGT Hospital, Gurugram, Haryana, India. The locale comprises rural communities and more than 80% of the population has very limited literacy or knowledge regarding drugs. Since only a small proportion of the population know about drugs, their role, use as well as misuse, it is entirely the clinician’s role and responsibility to educate and explain to the patients regarding proper use, dosage and follow up.
The process of conducting an audit of patient prescriptions from various departments in SGT hospital was an eye-opening experience for the staff that were a part of it. According to the calculated results of our study, we found that the patient’s details such as name, age and gender were 100% complete on the prescriptions. This could be due to the details being printed at the time of registration itself. Though addresses are also printed during registration, the noted absence of 4.5% (09/200) patient addresses in the obtained prescriptions might be due to factors such as; technical glitches during registration, absence of specific address in the hospital database or uninformed patient. The date of the appointment is also printed at the time of registration, but was still missing from 2.5% (05/200) of the prescriptions. This might also have been due to one of the aforementioned issues. Certain studies on auditing of hand-written prescriptions have reported that patient details were usually found to be incomplete in most prescriptions.2 Patient details are important as they ensure that correct patient receives the appropriate medicine and also important for record-keeping and medico-legal purposes. Whilst prescribing drugs with known contraindications or drugs for special populations, it is important to mention the age, gender and weight of the patient on the prescriptions.
Upon analysis of the results, we observed that the prescriptions written were incomplete with regards to the patient’s personal medical and surgical history, the patient’s family history and their clinical examination. The reasons could be a heavy OPD load, emergency cases in the ER, nonspecific complaints and tendency among clinicians for verbal communication rather than writing down in details. All prescriptions were missing with the details of contraindications regarding the medications and allergy status. A fraction of the prescriptions, about 12% (24/200) had clear initials of the prescribing clinician. The failure of stating the prescribers name is an example of ill practice and predisposes to future complications concerning patient’s having to re-visit, drugs being prescribed irrespective of the underlying disease and difficulty with tracing back for clarifications. Furthermore, initial details are important to identify the prescribing clinician, validate the authenticity of their prescriptions and hold them accountable for the medications they have prescribed. In a study similar to ours, the names of all the physicians and hospital addresses were printed on the prescriptions with doctor’s registration number and 17% of prescriptions did not have the physician’s initials.12 In the present study, out of the 200 prescriptions, 29.5% had diagnosis written in the prescriptions. A study from Merseyside, UK reported that 51% of their prescriptions (total, n= 81) didn’t have a diagnosis.13
Globally, untraceable to time or place, doctors have managed to gain a reputation for their illegible handwriting. In our study we found that 11.5% (23/200) of prescribing clinicians had illegible handwriting while 20% (40/200) had handwriting that was legible with difficulty. A similar type of study carried out in Delhi, India also reported that 15% of the prescribing doctors had illegible handwriting.14 Another study from Kerala, India reported that due to illegible handwriting of prescribing doctors, 3.4% (122/3557) medicines were unable to decode.15 These legibility issues can cause dispensing errors or administration errors which could lead to adverse drug reactions or adverse medical outcomes.16 To avoid such errors, the use of capital letters whilst prescribing drugs should be encouraged and where possible, switching to an electronic prescribing system is recommended.14 Prescription writing is regarded as one of the most important and basic skills which a doctor should be able to perform. Specific training and supervision for prescription writing must be emphasized during undergraduate and postgraduate training to minimize errors.17 A lack of accuracy and completeness in prescriptions with regards to all of the above-mentioned criteria could be due to lack of training but may also be influenced by the attitude of some doctors, who due to inadequate time, are unwilling to invest in writing clear and legible prescriptions. The extra time spent on the prescriptions, however, can avoid unnecessary enquiries from the pharmacist and also decrease discrepancies/delays in patient care with the intended drug therapy. In the guidelines laid down by the Medical Council of India, released on September 28, 2016 states that all drugs should be prescribed preferably in capital letters in legible handwriting and should also mention the generic name.18
In the present study, the average number of drugs prescribed (3.4±0.8) was higher when compared with the WHO laid benchmark i.e., two drugs per prescription.15 Similar studies from India reported higher average number of drug prescription (3.02±0.81 to 4.02±2.23 drugs).15,16 This indicator helps in measuring the practice of polypharmacy. The more the number of drugs prescribed, the more the chance of errors in healthcare cost and also there will be increase in the drug-drug interaction resulting in adverse drug reaction.14 The practice of drug prescription by generic names was found to be less prevalent (68.5%) in the present study which should ideally lie at 100%. This is in contrast studies by Anteneh and Ola et al., which reported the percentage of generic name drugs prescribed to be as high as 98.7% and 95.4%, respectively.6,7 Another study with almost similar results as ours by Sudarshan et al. also revealed the percentage of generic name drugs prescribed to be 69.26%20. Low prescription rates for generic name (45-55.4%) was reported in a similar type of studies from India.16,20 This may reflect the influential nature of pharmaceutical company representatives for inordinate favors. Prescribing generic drugs reduces the chances of errors while dispensing drugs which may be due to misinterpretation of sound-alike trade names of drugs and this will decrease the economic burden on the patients.21 The WHO considers generic drug prescriptions a safety precaution for the patients as it provides clear identification and enables for easy information exchange as well as for allowing better communication between health-care providers.6
We also observed that none of the prescriptions mentioned the allergy status of the patient. A study from North India also reported similar limitations on their study.16 Drug dose start date was mentioned in 98.6% (197/200) of the prescriptions whereas the duration of drug intake was mentioned amongst 50% (100/200) of the prescriptions. Strength of the prescribed drug was mentioned among only 27.14% (54/200) of the selected prescriptions. The absence of mentioning duration of drug intake may result in re-presentation to the physician due to treatment failure if the patient does not take the medication for the required course (i.e. in the case of antibiotics ± development of resistance)17 or adverse effects if the patient surpasses the recommended course duration. Most drugs which are available in variable strengths and dosage forms pose problems while dispensing, especially if trade/ brand names are used. Wrong dose, omission of dosage and wrong duration are the most common types of prescribing errors reported from most studies worldwide.22-24
In the present study, 61.5% of the prescriptions had a written instruction on the route of administration and oral route (88.6%) was the most common route mentioned in the prescriptions. A study from a teaching hospital in Kerala, India also reported oral route being the most common dosage form (87.4%) in their study.16 We observed that the percentage of injections per prescription was lower when compared with studies from India (7.54%) though both the findings are within the WHO laid limits (≤10%).16 The drug route instruction is very important as medication administration route has its own contraindications, which needs to be recognized by the treating doctor and the nurses involved. For example, in a patient with diarrhea or active rectal bleeding rectal route is contraindicated.25 The average consultation time in our study was 7.3±0.6 mins while other study reported lesser consultation time (average 2.8 min).14 Availability of EDL copy in all the OPDs in our study could be due to the continuous audit conducted by the Hospital Quality department for patient safety and improvement of healthcare quality. In our study, 51.5% (103/200) of the prescriptions had antimicrobials prescribed wherein only one antibiotic was mentioned amongst 40% (80/200) of the medicine cards, a combination of two antibiotics was mentioned in only 23/200 (11.5%) of the prescription. None of the prescriptions contained more than two antibiotics for any of the patients. This finding of antimicrobials prescription is higher when compared with the limits set by the WHO i.e., 20-25%.16 Studies from India reported higher antimicrobial prescription rates (39.01%->50%) which are also beyond the limits of the WHO.14,16 studies by Anteneh and Ola et al., combo-antimicrobial regimens (>2 antibiotics) were observed in 58.1% and 39.2 ± 8.8% respectively.6,7 a study by Sudarshan et al. it was found to be at a percentage of 39.4%.19 Polypharmacy was also quite prevalent in the above stated studies which increase the chances of adverse drug reactions, drug interactions as well as high expenses for the patient. It also leads to increased incidence of prescribing errors (those related to drug interactions).26 Use of antimicrobials should be rational as irrational use may lead to emergence of antimicrobial drug resistance, as well as increased adverse reactions and unnecessary hospital admissions6. Super infection is also a potential possibility with overprescribing of antimicrobials.5
Good clinicians must strive to create a systematic review of their day to day work, maintain proper record and assess the accuracy of the diagnosis made and also evaluate the outcome of their treatment. Assessment of the quality of medical care provided can be achieved by conducting PA as this provides documentary evidence. Extra time spent on the prescriptions, keeping in mind the correct framework and criteria, can decrease discrepancies/delays in patient care with the intended drug therapy and decrease adverse events related to prescription errors.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
ETHICS STATEMENT
The protocol of the study was approved by the institutional ethics committee of SGT University. Complete confidentiality of patients was maintained throughout the research process and informed written consent was obtained at initiation.
AVAILABILITY OF DATA
All data generated and analyzed during the present study are included in the manuscript.
- Bandyopadhyay D. A study of prescription auditing in a Tertiary Care Teaching Hospital of Eastern India. J Drug Delivery Ther. 2014;4(1):140-149.
Crossref - Solanki ND, Shah C. Prescription audit in outpatient department of multispecialty hospital in Western India: An observational study. Int J Clin Trials. 2015;2(1):14-19.
Crossref - Patterson HR. The problems of audit and research. J R Coll Gen Pract. 1986;36(286):196. PMID: 3746760
- Srishyla MV, Mahesh K, Nagarani MA, Sr. Mary C, Andrade C, Venkataraman BV. Prescription audit in an Indian hospital setting using the DDD (defined daily dose) concept. Indian J Pharmacol. 1994;26(1):23-28
- Rai S, Bhuvana K, Sowmya C, Sahana HV, Yaseen M. Prescription audit at a tertiary care teaching hospital. Natl J Physiol Pharm Pharmacol. 2018;8(9):1271-1274.
Crossref - Akl OA, El Mahalli AA, Elkahky AAA, Salem AMAA. WHO/INRUD drug use indicators at primary healthcare centers in Alexandria, Egypt. J Taibah Univ Med Sci. 2014;9:54-64.
Crossref - Desalegn AA. Assessment of drug use pattern using WHO prescribing indicators at Hawassa University teaching and referral hospital, South Ethiopia: A cross-sectional study. BMC Health Serv Res. 2013;13(1):170.
Crossref - Biswas NR, Jindal S, Siddiquei MM, Maini R. Patterns of prescription and drug use in ophthalmology in a tertiary hospital in Delhi. British J Clin Pharmacol. 2001;51(3):267-269.
Crossref - World Health Organization: How to Investigate Drug Use in Health Facilities: Selected Drug Use Indicators – EDM Research Series. http://apps.who.int/medicinedocs/en/d/Js2289e/.
- Afsan M, Alam MM, Noor N, Yousuf AKM, Haque MME. Audit of typical prescription format among the prescribers of a garment medical centre in Bangladesh. Update Dent Coll J. 2011;1:7-12.
- Pandey AA, Thakre SB, Bhatkule PR. Prescription analysis of pediatric outpatient practice in Nagpur city. Indian J Community Med. 2010;35(1):70-73.
Crossref - Janmano P, Chaichanawirote U, Kongkaew C. Analysis of medication consultation networks and reporting medication errors: A mixed methods study. BMC Health Serv Res. 2018;18(1):221.
Crossref - Smith R, Loh M, Mills D. Prescription audit. British Dental J. 2021;230 (4):189.
Crossref - Singh T, Banerjee B, Garg S, Sharma S. A prescription audit using the World Health Organization-recommended core drug use indicators in a rural hospital of Delhi. J Educ Health Promot. 2019;8:37.
Crossref - Dhanya TH, Sanalkumar KB, Andrews MA. Prescription auditing based on the World Health Organization (WHO) prescribing indicators in outpatient department of a teaching hospital in Kerala. Asian J Pharm Clin Res. 2021;14 (5):147-151.
Crossref - Ahsan M, Shaifali I, Mallick AK, Singh HK, Verma S, Shekhar A. Prescription auditing based on World Health Organization (WHO) prescribing indicators in a teaching hospital in North India. Int J Med Res Rev. 2016;4(10):1847-1852.
Crossref - Chaturvedi SK, Preeti S, Prabha SC, Geetha D. Improving quality of prescriptions with clinical audit. Indian J Med Sci. 2008;62(11):461-464.
Crossref - Prescribe generic medicines in capital letters: MCI. Times of India. https://timesofindia.indiatimes.com/city/aurangabad/Prescribe-generic-medicines-in-capital-letters-MCI/articleshow/54948409.cms. Accessed date October 16, 2016
- Sudarsan M, Sitikantha B, Aparajita D. Audit and quality assessment of prescriptions in an urban health Centre of Kolkata. Int J Med Public Health. 2016;6(3):136-139.
Crossref - Meenakshi R, Selvaraj N, Anandabaskar N, Dhamodharan A, Badrinath AK, Rajamohammad MA. Prescription audit of a teaching hospital in South India using World Health Organization core prescribing indicators – A cross-sectional study. Prespect Clin Res. 2021:
Crossref - Balbir K, Rani W. Prescription audit for evaluation of prescribing pattern of the doctors for rational drug therapy in a tertiary care hospital. J Drug Delivery Ther. 2013;3:77-80.
Crossref - Abidi A, Gupta S, Kansal S, Ramgopal. Prescription auditing and drug utilization pattern in a tertiary care teaching hospital of western UP. Int J Basic Clin Pharmacol. 2012;1(3):184-190.
Crossref - Seden K, Kirkham JJ, Kennedy T, et al. Cross-sectional study of prescribing errors in patients admitted to nine hospitals across North West England. BMJ Open. 2013;3:e002036.
Crossref - Kiekkas P, Karga M, Lemonidou C, Aretha D, Karanikolas M. Medication errors in critically ill adults: A review of direct observation evidence. Am J Crit Care. 2011;20(1):36-44.
Crossref - Kim J, De Jesus O. Medication Routes of Administration. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021. https://www.ncbi.nlm.nih.gov/books/NBK568677/
- Ndungu TK, Maru SM, Kuria KA, Karimi PN, Burburia JM. Prescription audit carried out at the pharmacy practice centre of the university of Nairobi between June and November 2004. East Cent Afr J Pharm Sci. 2007;10(2):51-55.
Crossref
© The Author(s) 2021. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.