


ISSN: 0973-7510
E-ISSN: 2581-690X
Interleukin-35 (IL-35), secreted mainly by T-regulatory cells (T-regs), has been considered to have immunosuppressive actions in many auto-immune diseases and tumors. However, information about its role in chronic hepatitis C (CHC) infection is still limited. We aimed to study the role of IL-35 within CHC infection and to assess its correlation with T-regs and T-helper 17 cells (Th-17). Therefore, we measured serum IL-35 concentrations using ELISA assay in 25 normal controls (NCs) and in 30 CHC patients before receiving direct antiviral agents (DAA) treatment and after 3 months of treatment end. T-regs and Th-17 cells frequencies were assessed via flow-cytometry in control group and patients’ group before treatment. The results showed that serum IL-35 levels revealed a highly significant increase in CHC patients compared to NCs (P <0.001). Moreover, IL-35 levels significantly decreased in patients 3 months after treatment end (P =0.02). Both Th-17 and T-regs were significantly increased in patients more than in NCs and a positive correlation was observed between them. However, T-regs/Th-17 ratio did not show significant difference from the ratio in NCs. IL-35 levels were positively correlated with viral load and T-regs frequency, but not with Th-17 frequency. IL-35 levels did not correlate with liver enzymes or functions. These results suggested that IL-35 enhances the immunosuppressive functions of T-regs, protecting the liver from HCV induced damage and contributes to viral persistence. IL-35 may represent a possible immunotherapeutic strategy for chronic persistent infection if given with DAA, especially in relapsing or non-responding cases.
HCV, CHC, Interleukin 35, immunosuppressive cytokines, T helper 17 cells, T regulatory cells
CHC infection leads to a range of liver disorders, ranging from asymptomatic mild inflammation to severe fibrosis, subsequent cirrhosis and hepatocellular carcinoma, causing significant morbidity as well as mortality to the affected patients1. HCV and its complications are considered significant public health problem that Egypt has to challenge as the highest prevalence of HCV infection in the world was recorded in Egypt up to 14.7 % in 2015 and the most common isolated genotype is HCV genotype 4, in about 90% of CHC patients in Egypt2.
Although HCV exhibits a non-cytopathic activity in the liver, the primary cause of liver damage is immune-mediated destructive reactions of the host immune response against the virus2,3. If host T-cells display vigorous constant responses, HCV might be eliminated spontaneously in early disease, however, the infection will be chronic if the response of T-cells is fragile or temporary4. In addition, in acute infection with HCV if CD4+ Th-1 cells produce intensive interferon -c, IL-2 alongside the active macrophages and CD8+ T cells response, the virus will be effectively eliminated more than in patients with predominant Th-2 response which produce interleukins 4,5,10 and 135. Moreover, CD4+ T cells may differentiate to subsets rather than Th-1 and Th-2 subsets, as CD4+CD25+foxp3+ T-regs, which secrete IL-10 and transforming growth factor-β1 (TGFβ1), to suppress antiviral immune responses and control inflammatory liver damage, leading to viral persistence and immune tolerance in CHC6. Th-17 is another CD4+ T cells subset that secretes proinflammatory cytokines as interleukins 17A, 17F and 227. If imbalance occurs between T-regs and Th-17, many disorders as autoimmune diseases, chronic inflammations as well as tumors will occur and progress8.
IL-35 is the latest member defined in the IL-12 family and greatly expressed in T-regs. Other cells such as vascular endothelial cells, smooth muscle cells and monocytes may express it during inflammation9. IL-35 is considered to have immunosuppressive action by enhancing T-regs cells proliferation and suppressing Th-17 cells differentiation10. Hence, IL-35 can contribute to persistent HCV infection through suppressing immune response against the virus. Meanwhile, it can prevent HCV-induced liver injury by inhibiting pro-inflammatory cytokines expression11.
A significant improvement in viral clearance and sustained viral response (SVR) was observed in patients treated with DAAs more than in patients treated with ribavirin and pegylated interferon combination therapy12. However, many further concerns to challenge with are found, as immune tolerance, immune exhaustion, fibrosis and severe liver injury as well as viral relapse, all of which require more study. Limited studies have been conducted on IL-35 in CHC infection so far. The regulatory potential of IL-35 makes it an attractive target for therapeutic intervention as an immunosuppressive factor, therefore recombinant IL-35 or IL-35-producing cells may be used alongside antiviral drugs to protect liver from HCV-induced injury.
In this study we aimed to assess the change in serum IL-35 concentrations in CHC infected patients before starting treatment and after 3 months of treatment end. In addition, we studied the possible association of IL-35 with T-regs and Th-17 frequency and other laboratory parameters, in order to explore its role in HCV chronic infection.
Patients and Methodology
Subjects
The present study is an observational cross-sectional study conducted on patients visiting the outpatient clinic of the Virology unit, Faculty of Medicine, Ain Shams Research Institute, Ain shams University Hospital (MASRI), Cairo, Egypt, in the period from September 2018 to September 2019. It included thirty patients diagnosed as having CHC class A based on Child-Turcotte-Pugh (CTP) classification (Group 1) and twenty five apparently healthy subjects (Group 2) tested negative for HCV antibody. The thirty patients were twenty males and ten females. The mean age of patients was 44.97 years (±13.79) ranging from 27 to 78 years. As regard normal controls they were 15 males and 10 females. Their mean age was 32.8 years ± 7.45 ranging from 25 to 55 years. Before collecting samples, Informed consents were taken from all participants, in accordance to the “regulation of the Ethical Committee of Scientific Research of Faculty of Medicine, Ain Shams University, Cairo, Egypt” and according to “The Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments in humans”.
Inclusion criteria
The study included CHC class A patients. They were positive for anti-HCV antibody (ELISA kit; Biotech Co., LTD, Turkey) for at least six months. All patients were naive treatment (did not receive any antiviral treatment) when the samples were collected.
Exclusion criteria
Patients presented with end-stage liver diseases (CTP class B or C or hepatocellular carcinoma) or started antiviral treatment or immune-modulatory therapies and/ or had other hepatitis viruses co-infection were excluded from the study.
The study method briefly included the following steps:
- Full history taking and clinical data collection
- Blood samples collection from control group and from CHC patients group before treatment and 3 months after treatment end
- IL-35 were measured in healthy controls and in CHC patients group before treatment and 3 months after treatment end using direct ELISA technique
- Tregs and Th17 cells were measured in NC and in CHC patients group before treatment using Flow cytometric analysis
- Data analysis
All the enrolled patients were subjected to:
Full history taking
Thorough clinical examination and routine laboratory investigations for chronic viral hepatitis, including liver functions testing (total bilirubin, albumin, prothrombin time), liver enzymes (ALT & AST), complete blood count (CBC) and quantitative RT- PCR for HCV. Then, blood samples were obtained before treatment and after 3 months of treatment end. The treatment protocol given was sofosbuvir 400mg/day and daclatasvir 160 mg/day for 12 weeks, according to Egyptian protocol of treatment13.
Estimation of serum IL-35
The serum IL-35 levels were measured in blood samples of patients before starting treatment and 3 months after treatment end as well as in NC group blood samples, using a commercially available quantitative sandwich ELISA technique (Biotech Co., LTD, Turkey) following the manufacturer’s instructions. Optical densities were read using a micro-plate reader (CLARIOstar®, BMG Labtech., Germany) within 10 min of adding stop solution at 450 nm. The detection limit was 0.27 ng/mL.
III- Flowcytometric assay of T-regs as well as Th-17 among Peripheral blood mononuclear cells
T-regs and Th-17 frequency were measured in blood samples of patients group (3 ml in EDTA tube) before treatment as well as in control group blood samples, using flow-cytometric analysis as follows:
Peripheral blood mononuclear cells (PBMCs) were taken from the peripheral blood using Ficoll-Hypaque density centrifugation “3000 r/min for 10 minutes at room temperature”, then T-regs were purified using fluorescein-isothiocyanate (FITC) antihuman CD4 (Beckman-Coulter Co., USA), phycoerythrin (PE) antihuman CD25 (Beckman-Coulter Co., USA) as well as phycoerythrin cyanine antihuman CD127-PC5 (Beckman-Coulter Co., USA). In Addition, Th-17 were purified using PE-antihuman CD3 (Beckman-Coulter Co., USA), PC5-antihuman CD4 (Beckman-Coulter Co., USA) as well as FITC-antihuman IL-17-A (Bio-techne. Co., Turkey) according to the manufacturer’s instructions. All labeled samples were tested through NAVIOS flow cytometer using the NAVIOS CXP software (Navios Tetra, Navios Win 7 Workstation) (Beckman Coulter Co., USA). In order to exclude positive and negative cells, isotype control antibodies were used in the PE, FITC and PC5 fluorescence channels then the activated phenotype of T-regs was defined as CD4+CD25+CD127dim/−cells (Fig. 1) and Th-17 cell was identified as CD3+CD4+ IL-17A+ cells (Fig. 2).
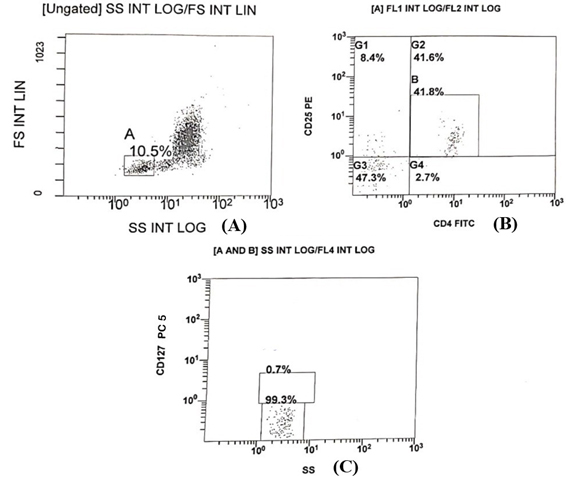
Fig.1. lymphocytes stained with anti-CD4 FITC, anti-CD25 PE and anti CD127 PC5: (A) dot blot of forward scatter (FS) versus SS (side scatter) shows lymphocytes gate A which represent 10.5 % of the harvested cell populations. (b) A dot plot of anti-CD25 PE versus anti-CD4 FITC shows that 41.8 % of the gated lymphocytes populations were CD4+CD25+, a gate G2 included this population. (c) CD4+CD25+ lymphocytes were examined for expression of CD127. the dot blot demonstrates that 99.3% of the CD4+CD25+ lymphocytes population did not express or fairly express CD127 So, activated T-regs percentage was 41.5% in this sample as T-regs were defined as CD4+CD25+CD127dim/−cells

Fig.2. lymphocytes stained with anti CD3 PE, CD4 PC5 and anti IL-17A FITC 1. dot blot of forward scatter (FS) versus SS (side scatter) shows lymphocytes gate A which represent 14% of the harvested cell populations. 2. (b) A dot plot of anti CD3 PE against anti CD4 PC5 shows that 30.4 % of the gated lymphocytes populations were CD3+CD4+, a gate G2 included this population 3. CD3+CD4+ lymphocytes were examined for expression of IL-17A FITC, the dot blot demonstrates that 70% of the CD3+CD4+ lymphocytes population express high levels of IL-17A as shown in figure 2-(C) So, Th-17 percentage was 20.68 % of the total lymphocytes in this sample as Th-17 cells were identified as CD3+CD4+ IL-17A+ cells.
Data assessment
Data analysis was performed using statistical program for social science (SPSS) version 23 as follows: for describing the considered sample, quantitative data were presented as minimum, maximum, mean and standard deviation (median and IQR for non-parametric data). Qualitative data were exhibited as count and percentage. For comparing quantitative data between two groups, Student “t” test was used when comparing non-parametric data, Mann Whitney U test was used. Pearson’s and Spearman’s correlation tests were performed to measure correlation between different continuous variables. P-value < 0.05 is considered statistically significant.
The laboratory investigations done for the patients are listed in table (1). A significant decrease was observed in ALT, AST and total bilirubin while a significant elevation was found in serum albumin level among patients 3 months after treatment end, in comparison to their levels before treatment. All patients achieved SVR 3 months after treatment end (negative quantitative RT-PCR).
Table (1):
Patients laboratory investigations done before treatment and 3 months after treatment end.
| Mean (±SD) | P-valuea | ||
|---|---|---|---|
| ALT (IU/L) | Before TTT | 51.69 (24.9) | <0.001 |
| 3 months after TTT end | 31.10 (18.8) | ||
| AST (IU/L) | Before TTT | 42.45 (38.1) | 0.03 |
| 3 monthsafter TTT end | 26.24 (20.7) | ||
| T bil (mg/dl) | Before TTT | 0.74 (0.24) | 0.01 |
| 3 months after TTT end | 0.56 (0.33) | ||
| ALB (g/dl) | Before TTT | 4.08 (0.61) | 0.01 |
| 3 months after TTT end | 4.29 (0.57) | ||
| Quantitative PCR b (IU/ml) | Before TTT | Median: 967766.5 IQR: 381590-2556215 |
|
| 3 months after TTT end | Negative |
A comparison between different laboratory parameters performed for CHC patients before and after treatment with DAAs. a There was highly significant statistical difference (P value ≤0.05) in the levels of ALT, AST, total bilirubin and serum albumin levels before and after 3 months of DAAs treatment. b All the patients enrolled achieved sustained virological response after 3 months of treatment end, confirmed by a negative PCR. ALB: albumin, ALT: alanine-transaminase, AST: aspartate-transaminase, HS: highly significant, IQR: interquartile range, PCR: quantitative polymerase chain reaction, S: significant, T bil: total bilirubin, TTT: treatment.
IL-35 serum level
IL-35 serum levels in CHC patients showed highly significant increase (18.77± 11.91 ng/mL) compared to 2.01± 1.38 ng/ mL in NC (P value <0.001; Table 2). Serum IL-35 levels were significantly declined after achieving SVR (3 months after treatment end) to reach 7.91±9.63 ng/ml (P value <0.001) as shown in Fig. 3.
Table (2):
Serum IL-35 level, T-regs and Th-17 frequency and Tregs/Th-17 ratio in patients and controls.
| Patients | Control | P-value | |
|---|---|---|---|
| Mean (±SD) | Mean (±SD) | ||
| IL-35 (ng/ml) | 18.8 (11.9) | 11.9 (1.4) | <0.001 HSa |
| T-regs (%) | 23.4 (11.4) | 11.4 (0.8) | <0.001 HSa |
| Median (IQR) | Median (IQR) | ||
| Th-17 (%) | 6.3 (9.4) | 0.4 (0.4) | <0.001 HSa |
| T-regs/TH-17 Ratio | 3.8 (2.2-5.5) | 3.6 (2.1-5.2) | <0.001 NSb |
A There was a highly statistically significant difference in serum IL-35 level, Tregs and Th17 cells percentages between CHC patients and healthy controls (P-value ≤0.05), b while there was no statistical difference in Tregs-Th17 ratio among the two groups. HS: highly significant, IL-35: interleukin 35, NS: non-significant, Th-17: T helper 17 cells, T-regs: T regulatory cells.
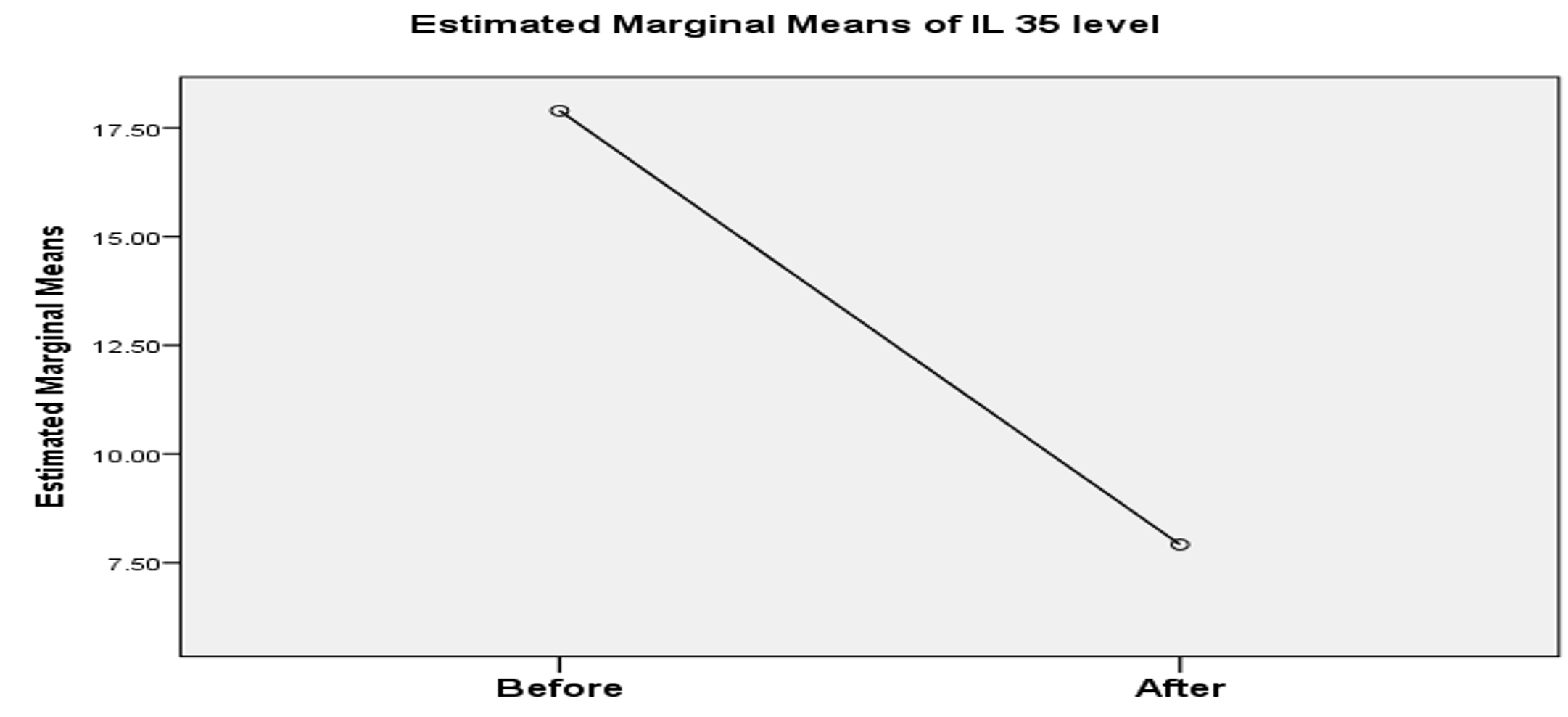
Fig. 3. Comparison between IL-35 levels in serum among patients before treatment and 3 months after treatment end.
A statistically positive correlation was observed between the serum IL-35 level and the viral load among CHC patients before treatment (P value = 0.02). Serum IL-35 levels before and 3 months after treatment end showed insignificant correlation with liver enzymes or liver functions, except for serum albumin level which showed a positive correlation with serum IL-35 level 3 months after treatment end (P value= 0.02) as shown in table 3.
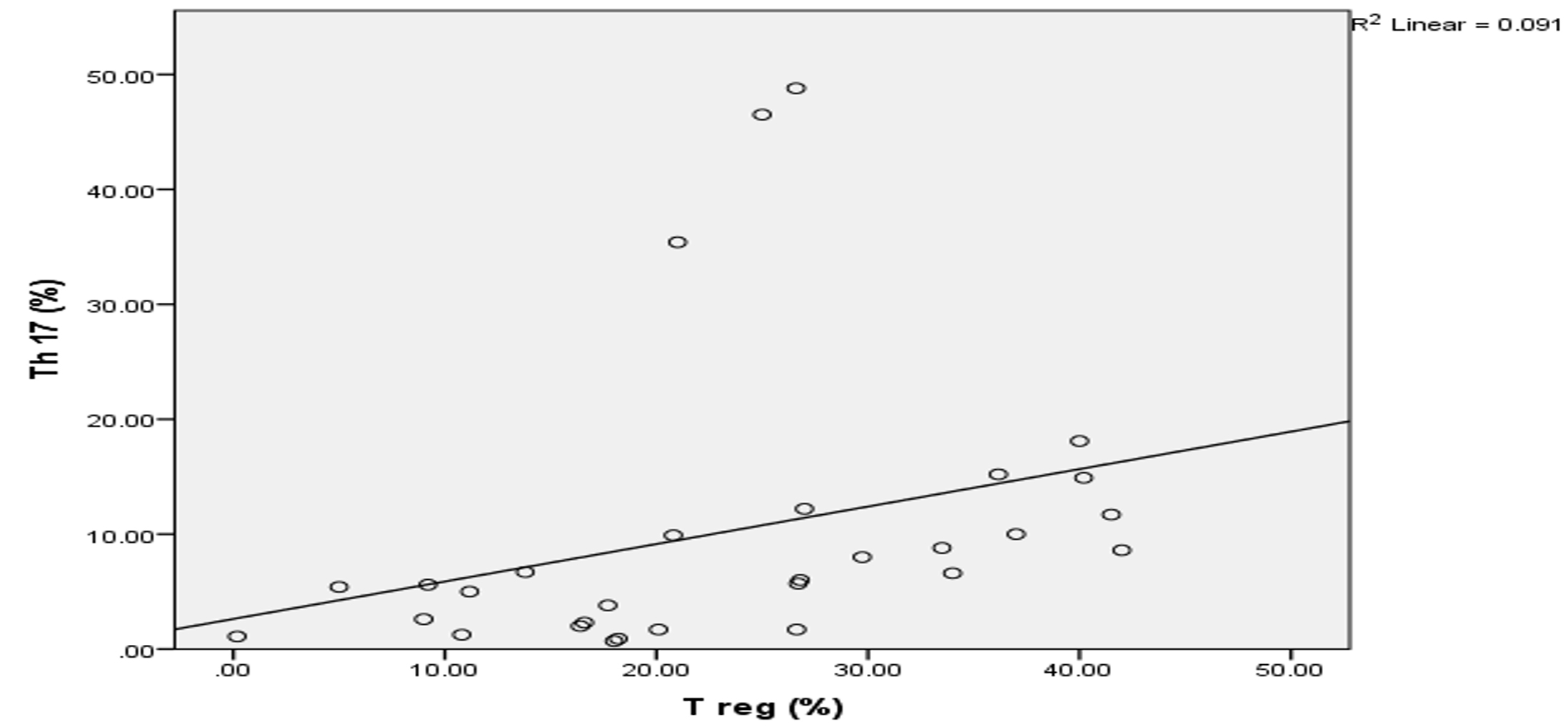
Fig. 4. Correlation between T-regs and Th-17 cells frequencies among CHC patients before treatment.
Table (3):
Correlation between IL-35 and laboratory work-up.
| IL-35 before treatment | IL-35 three months after treatment end | |
|---|---|---|
| P- value | ||
| ALT (IU/L) | 0.95 NS b | 0.38 NS b |
| AST (IU/L) | 0.84 NS b | 0.81 NS b |
| Tbil (mg/dl) | 0.38 NS b | 0.18 NS b |
| ALB (g/dl) | 0.82 NS b | 0.02 S a |
| Quantitative PCR (IU/ml) | 0.02 S c | |
a,b Serum IL-35 levels before and 3 months after treatment end showed insignificant correlation with liver enzymes or liver function tests, except for serum albumin level, which showed a positive correlation with serum IL-35 level 3 months after treatment end (P value < 0.05). cA statistically positive correlation was observed between the serum IL-35 level and the viral load among CHC patients before treatment (P value < 0.05). ALB: albumin, ALT: alanine-transaminase, AST: aspartate-transaminase, IL-35: Interleukin 35, NS: non significant, PCR : polymerase chain reaction, S: significant, Tbil: total bilirubin.
T-regs and Th-17 cells frequency
T-regs percentage among patients was 23.36 % ±11.43, compared to 1.65% ± 0.78 in NC. Th-17 percentage has 6.30% median with 9.40 IQR, compared to 0.40% median with 0.40 IQR in NC. T-regs and Th-17 percentages in patients showed highly significant increase than their percentages in NCs (P value < 0.001) as shown in Table 3. The Tregs/Th-17 ratio did not show significant statistical difference from those found in NC (Table 2). A highly significant positive correlation was observed between T-regs and Th-17 cells frequencies among CHC patients (P value<0.001) as shown in Fig. 4. In addition, patients’ serum levels of IL-35 before treatment had a significant positive correlation with T-regs frequency, while it had no significant correlation with Th-17 percentage. On the other hand, there was no significant correlation between the frequency of either T-regs or Th-17 cells with any of the laboratory parameters performed as shown in table 4.
Table (4):
Correlation between T-regs and TH-17 frequency and laboratory investigations parameters.
| T-regs (%) | Th-17 (%) | ||
|---|---|---|---|
| P valuea | |||
| ALT (IU/L) | 0.27 NS | 0.40 NS | |
| AST (IU/L) | 0.71 NS | 0.11 NS | |
| Tbil (mg/dl) | 0.26 NS | 0.15 NS | |
| ALB (g/dl) | 0.11 NS | 0.44 NS | |
| Quantitative PCR (IU/ml) | 0.12 NS | 0.48 NS | |
a Analyzing the correlation between T-regs and Th17 cells with different laboratory parameters performed to the enrolled patients revealed a non-significant correlation between either of the two cells and these lab parameters (P values <0.05). ALB; albumin, ALT: alanine-transaminase, AST: aspartate-transaminase, NS: non-significant, PCR: quantitative polymerase chain reaction, Tbil; total bilirubin, Th-17: T helper 17 cells, T-regs: T regulatory cells.
HCV is one of the primary reasons for chronic hepatitis, liver fibrosis, liver cirrhosis, hepatocellular carcinoma worldwide and it is a leading cause for liver transplantation in developed countries14. Infection with HCV is considered a significant health issue in Egypt as the highest prevalence of HCV infection in the world was recorded in Egypt about 14% in 20152. Many studies reported that HCV does not have cytopathic effect on the liver and HCV related liver injury is purely immune-mediated as a result of a complicated host immune response2,11. T regs and Th-17 cells have been revealed to play a vital role during chronic inflammatory disorders15. IL-35 has been demonstrated to induce immunotolerance in immune-mediated diseases11. The IL-35 role in CHC was still incompletely elucidated. Thus, the current study aimed to assess its role in CHC infection.
All cases enrolled in the study achieved SVR 3 months after treatment end. The SVR was associated with improvement in liver inflammation and function. The same results were reported by other studies16-19. Foster et al. 16 found that viral clearance was achieved in 81.6% of treated decompensated cirrhosis patients, with improvement in liver function and liver enzymes , whereas liver functions were worsened and liver enzymes remained elevated in untreated patients. Abozeid et al. 19 found that DAAs treatment was associated with SVR in about 95.1% of patients enrolled in their study, with improvement in transaminases and bilirubin level by the end-of-treatment. In the same venue, other studies17,18 found that DAAs treatment was associated with SVR rate above 92% and they revealed an unexpected improvement in liver function with significant decline of ALT and AST in treated patients. The viral clearance occurring after DAAs administration leads to decrease in the intrahepatic immune-mediated inflammation and hepatocytes damage with significant improvement in liver functions as the intrahepatic inflammation directly reduces the synthetic capacity of the liver, thus after virus clearance and blocking inflammation, the liver function can be restored to some extent11,17.
The present study showed that serum IL-35 levels revealed a highly significant increase in CHC patients group more than its levels in control group. In addition, there was a significant decline in the IL-35 levels in all patients after receiving DAA and achieving SVR. This comes in accordance with other studies11,20,21.
The higher IL-35 level in patients and its decline after treatment suggest its pivotal role in the immunopathogenesis of HCV infection, especially in persistent chronic HCV infection, and a possible correlation with liver inflammation. Whether these higher levels mean it is an immunosuppressive cytokine or an immune-stimulant one is a raised question.
Serum IL-35 levels were positively correlated with HCV viral load. This finding goes in accordance with Liu et al.11 and Shao et al.20, who observed the same result as they reported that IL-35 was elevated in the serum of patients with CHC compared to that in healthy individuals and treatment led to significant decline in IL-35 concentration as well as the viral load. In addition, Liu et al.11 found that IL-35 didn’t have direct antiviral effects against HCV in cultured cells after direct IL-35 stimulation. In their study, a total of 107 copies of HCV in cell culture (HCV cc) were added to cell culture (Huh7.5 cells) for 5 h, then incubated with and without recombinant IL-35(rIL-35) for 48 hours (final concentration of 1ng/ml). HCV RNA replication in both cultured cells and supernatants was determined using RT-PCR. The levels of HCV RNA did not show significant differences in response to rIL-35 in either the HCVcc-infected Huh7.5 cells or the supernatants from cultured cells.
The positive correlation found between viral load and IL-35 could be explained by the possible immunosuppressive function of IL-35. Whenever the virus replicates and causes immune-mediated liver injury, the more immune suppression factors are activated to lessen the damage and impairment, i.e. IL-35 increases to suppress antiviral immune responses and to reduce inflammatory responses leading to viral persistence in chronic viral hepatitis11,20,21.
On the contrary, Shi et al.20 reported that no correlation was observed between HBV DNA loads and IL-35 in peripheral blood. However, they suggested a probable anti-inflammatory effect of IL-35 to limit liver damage without directly inhibiting viral replication and that the viral load in peripheral blood might not reflect those inside the liver tissue.
Many studies directed on the T-regs role during infection with HCV11-22. The major function of T-regs is to control the immune response of T cells against pathogens, tissue damage and severe inflammation as well as T-regs regulate the balance of the immune responses. T-regs primarily act through soluble cytokines secretion as IL-10, transforming growth factor -β1 and IL-3522. The occurrence and development of CHC are associated with changes in the T-regs frequency11.
The current study found that T-regs percentages exhibited a highly significant increase among patients in comparison to NC (P. < 0.001). This finding comes in accordance with other studies conducted in CHC and CHB patients11,21,23-25. The increase in T-regs percentages in peripheral blood might be caused by the inflammation and necrosis of the liver tissue during HCV and/or HBV infection that induce the production of T-regs as immunosuppressant cells to prevent extensive liver damage. This immunosuppressive function may cause infection to become chronic in most of the patients25,26.
On the other hand, Claassen et al.26 reported that CHC did not change the blood cellularity and numbers of T-regs might be declined as compared to normal healthy controls. The definite number as well as the fraction of these T-regs to lymphocytes was lesser in CHC patient blood than in healthy subjects blood. In addition, the authors found high numbers of T-regs inside the HCV infected liver, while they were absent from healthy liver. This discrepancy may be explained by localization of differentiated and highly activated T-regs in large numbers inside chronic HCV infected liver 27.
Th-17 cells share the T-regs origin from the same naive T cells and have similar signaling differentiation pathways. Opposing the action of T-regs, Th-17 cells up-regulate inflammation. More importantly, the imbalance between T-regs and Th-17 is expected to be responsible for viral persistence in CHC and CHB infections7. If the ability of T-regs to suppress Th-17 response is enhanced, the balance of T-reg/Th-17 would be skewed towards T-reg cells, hence regulating the liver tissue injury and even prevent the disease progression24.
Few studies were conducted on Th-17 cells in CHC patients, while it was extensively studied in CHB, therefore we investigated Th-17 cells frequency in CHC patients. Higher significant levels of Th-17 among patients were noticed in comparison to controls (P value <0.001). This significant increase agrees with other studies15,28-30. Chang et al.28 found that there was a significantly higher frequency of circulating Th17 cells in CHC patients compared to normal controls. In addition,Yang et al.15 showed a highly increased HBV core-specific Th17 cell response in CHB patients when compared with asymptomatic carriers. As well as Yang et al.30 observed significantly higher frequencies of the circulating Th17 cells in patients with CHB, cirrhosis and liver failure compared with levels in the normal controls. The significant elevation of Th-17 frequency in CHC and CHB patients illustrates the vital role of Th-17 in triggering liver inflammation through production of pro-inflammatory cytokines such as interleukins (17 and 22)31. On the contrary, other studies31,24 did not declare any statistically significant difference in the Th-17 cells frequency in CHC patients’ peripheral blood, although significantly higher numbers of Th-17 inside the liver were observed compared to its frequency in peripheral blood samples.
Th-17 cells might settle inside the liver and therefore, circulating IL-17 cells levels might not significantly increase peripherally16. The discordance between the current study results and other studies may be explained by conducting the studies on patients with different stages of CHC infection, as the Th-17 trapping in liver tissue may occur in disparity proportion in different stages of CHC infection16.
The current study revealed a highly significant positive correlation between T-regs and Th-17 frequency in the patients group. The T-regs/Th-17 ratio did not significantly differ from the ratio in HCs. Same findings were reported by other studies15,24,32-34. It may be due to the simultaneous increase in both cells in CHC patients.
The correlation between T-regs, Th-17 frequency and IL-35 in CHC patients was analyzed by the current study. It was revealed a significant positive correlation between T-regs frequency and IL-35, but it did not find any significant correlation between Th-17 frequency and IL-35.
Previous studies11,15,20,21 found that IL-35 levels in serum were increased in CHB and CHC patients as well as asymptomatic carriers, enhancing the suppressive functions of T-regs and reducing other CD4+ T cells and cytotoxic CD8+ T cells activities. An in vitro study by Collison et al.35 reported that T cells exposed to IL-35 directly can generate a new kind of T-regs (iTr35) that are distinct from IL-10 or TGF-β induced T-regs. These iTr35 kind of cells mediate a stronger immune-suppressive activity in infections and tumors than IL-10 or TGF-β induced T-regs. The generation of the iTr35 cells can be stimulated by IL-35 as well as further IL-35 is additionally secreted by these cells, generating a positive feedback loop35. As well as, Liu et al.11 investigated the regulatory role of IL-35 on T-regs in peripheral blood monocytes from CHC patients and healthy individuals stimulated with recombinant IL-35 (rIL-35) for 6 h. They found that the IL-35 stimulation not only elevated the percentage of T-regs in CHC patients, but also up-regulated the production of anti-inflammatory cytokines (e.g., IL-10 and IL-35) and inhibited other cells proliferation, which indicates enhancement of the suppressive function of Tregs. They also observed that rIL-35 stimulation increased FoxP3 mRNA expression in T-regs of CHC patients. In CHB infection, Shao et al.20 found that IL-35 stimulation in T-regs co-culture system not only inhibited other cellular proliferation, but also up-regulated the production of IL-10 and IL-35. Furthermore, Yang et al.15 studied the role of regulatory function of IL-35 to viral specific Tregs/Th17 cells balance in chronic HBV infection in vitro. rIL-35 stimulation elevated Tregs frequency, FoxP3 mRNA relative level and IL-10 production. However, there was no remarkable differences of viral specific Th17 cells and RORγt mRNA in response to rIL-35 stimulation and the ratio of Tregs/Th17 was remarkably elevated in response to IL-35 stimulation. As regard the secreted cytokines, IL-10 expression was elevated in response to rIL-35 stimulation, while IL-17 production by CD4+ T cells was down-regulated with IL-35 stimulation in comparison of presence and absence of IL-35 treatment. These in vitro studies’ results suggest that IL-35 contributes to suppressing the immune responses against the virus as well as lessening the inflammatory activity in CHB and CHC infections, mainly through enhancing the Tregs suppressive function In addition, IL-35 regulation to viral specific Tregs/Th17 balance may contribute to viral persistence in CHC and CHB infection11,15.
In acute HBV infection, Teng et al.36 revealed that IL-35 level was significantly increased in patients’ peripheral blood as well as Th-17 cells frequency was increased but negatively correlated with IL-35 serum levels. In addition, the IL-35 suppressed Th-17 cells differentiation from CD4+ T cells and decreased Th-17 cytokines production in vitro as well as in vivo, suggesting the crucial role of IL-35 in regulating the peripheral and hepatic Th-17 cells in vivo and in vitro, which may consequently modulate liver injury and hepatocyte inflammation during acute infection with HBV36.
Differences in results of previous studies may be attributed to different numbers of included patients, distinct clinical stages of CHC, the extent of histological liver damage and infection severity and duration, as well as different geographical distribution of the prevalent viral genotype.
The current study showed that serum IL-35 levels significantly increased in CHC patients compared to NCs (P <0.001). Moreover, IL-35 levels significantly decreased in patients 3 months after treatment end (P =0.02). Both Th-17 and T-regs were significantly increased in patients more than in NCs and a positive correlation was observed between them. Moreover, IL-35 levels were positively correlated with viral load and T-regs frequency, but not with Th-17 frequency. As well as, IL-35 levels did not correlate with liver enzymes or functions. These results suggest that the IL-35 enhances immunosuppressive functions of T-regs so it may protect the liver from HCV induced damage and contribute to viral persistence. Therefore, the regulatory potential role of IL-35 makes it an attractive target as immunotherapeutic strategy in treating chronic persistent infections such as CHC, along with other antiviral drugs to protect the liver from the virus induced damage, specially in relapsing or non-responding cases to DAAs.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors have made substantial contributions to conception and design of the study. HIA and SSA contributed to samples collection and acquisition of patients’ data. HIA performed examination of the patients and diagnosed the cases. AEA and SSA contributed to all laboratory work with analysis and interpretation of data. DME, AEA, HIA and SSA contributed to drafting the article. SEB and DME contributed to revising the draft critically for important intellectual and scientific content. OAA revised the clinical content. All authors provided final approval of the version to be published.
FUNDING
None.
ETHICS STATEMENT
The study was carried out in accordance to the recommendations of the Ethical Committee of Scientific Research of Faculty of Medicine, Ain Shams University, Cairo, Egypt (FWA000017585/ MD 75/2018) and according to The Code of Ethics of the World Medical Association (Declaration of Helsinki) for experiments on humans.
AVAILABILITY OF DATA
All datasets generated or analyzed during this study are included in the manuscript.
- Petruzziello A, Marigliano S, Loquercio G, Cozzolino A, Cacciapuoti C. Global epidemiology of hepatitis C virus infection: an up-date of the distribution and circulation of hepatitis C virus genotypes. World J Gastroenterol. 2016;22(34):7824-7840.
Crossref - Elkhawaga AA, Hosni A, Zaky DZ, Kamel AA, Mohamed NA, Abozaid MA, El-Masry MA. Association of Treg and TH17 Cytokines with HCV Pathogenesis and Liver Pathology. Egyptian J immunology. 2019;26(2):55-63. PMID: 31926495.
- Dustin, LB, Bartolini B, Capobianchi MR, Pistello M. Hepatitis C virus: life cycle in cells, infection and host response, and analysis of molecular markers influencing the outcome of infection and response to therapy. Clin Microbiol and Infect. 2016;22(10):826-832.
Crossref - Irshad M, Mankotia DS, Irshad K. An insight into the diagnosis and pathogenesis of hepatitis C virus infection. World J Gastroenterology. 2013;19(44):7896-7909.
Crossref - Chalupa P, Holub M, Davidova A, Arientova S, Beran O. Immune response in pathogenesis of hepatitis C viral infection. Epidemiol Microbiol Immunol. 2015;64(4):198-203.
- Jung MK, Shin EC. Regulatory T cells in hepatitis B and C virus infections. Immune Netw. 2016;16(6):330-336.
Crossref - Xue-Song L, Cheng-Zhong L, Ying Z, Mo-Bin W. Changes of Treg and Th17 cells balance in the development of acute and chronic hepatitis B virus infection. BMC Gastroenterol. 2012;12(1):43.
Crossref - Hanidziar D, Koulmanda M. Inflammation and the balance of Treg and Th17 cells in transplant rejection and tolerance. Curr Opin Organ Transplant. 2010;15(4):411-415.
Crossref - Ye S, Wu J, Zhou L, Lv Z, Xie H, Zheng S. Interleukin-35: the future of hyperimmune-related diseases? J Interferon Cytokine Res. 2013;33(6):285-291.
Crossref - Barnes PJ. Immunology of asthma and chronic obstructive pulmonary disease. Nat Rev Immunol. 2008;8(3):183-192.
Crossref - Liu S, Zhang Q, Shao X, Wang W, Zhang C Jin Z. An immunosuppressive function of interleukin-35 in chronic hepatitis C virus infection. International Immunopharmacology. 2017;50:87-94.
Crossref - Feld JJ, Jacobson IM, Hezode C, et al. Sofosbuvir and velpatasvir for HCV genotype 1, 2, 4, 5, and 6 infection. N Engl J Med. 2015;373(27):2599-2607.
Crossref - El-Akel W, El-Sayed MH, El Kassas M, et al. National treatment programme of hepatitis C in Egypt: Hepatitis C virus model of care. J Viral Hepat. 2017;24(4):262-267.
Crossref - Quer J, Mur JIE. In: Thomas HC, Lok AS, Locarnini SA, Zuckerman A, editors. Viral Hepatitis. Oxford: Wiley Blackwell. 2014;246-65.
- Yang L, Jia S, Shao X, et al. Interleukin-35 modulates the balance between viral specific CD4+ CD25+ CD127dim/- regulatory T cells and T helper 17 cells in chronic hepatitis B virus infection. Virol J. 2019;16(1):1-10.
Crossref - Foster GR, Irving WL, Cheung MC, et al. Impact of direct acting antiviral therapy in patients with chronic hepatitis C and decompensated cirrhosis. J Hepatol. 2016;64(6):1224-1231.
Crossref - Mohamed MS, Hanafy AS, Bassiony MA, Hussein S. Sofosbuvir and daclatasvir plus ribavirin treatment improve liver function parameters and clinical outcomes in Egyptian chronic hepatitis C patients. Eur J Gastroenterol Hepatol. 2017;29(12):1368-1372.
Crossref - Elsharkawy A, Eletreby R, Fouad R, et al. Impact of different sofosbuvir based treatment regimens on the biochemical profile of chronic hepatitis C genotype 4 patients. Expert Rev Gastroenterol Hepatol. 2017;11(8):773-778.
Crossref - Abozeid M, Alsebaey A, Abdelsameea E, et al. High efficacy of generic and brand direct acting antivirals in treatment of chronic hepatitis C. Int J Infect Dis. 2018;75:109-114.
Crossref - Shao X, Ma J, Jia S, Yang L, Wang W, Jin Z. Interleukin-35 suppresses antiviral immune response in chronic hepatitis B virus infection. Front Cell Infect Microbiol. 2017;7:472.
Crossref - Shi YY, Dai MJ, Wu GP, Zhou PP, Fang Y, Yan XB. Levels of interleukin-35 and its relationship with regulatory T-cells in chronic hepatitis B patients. Viral immunology. 2015;28(2):93-100.
Crossref - Lina C, Conghua W, Nan L, Ping Z. Combined treatment of etanercept and MTX reverses Th1/Th2, Th17/Treg imbalance in patients with rheumatoid arthritis. J Clin Immunol. 2011;31(4):596-605.
Crossref - Yoshizawa K, Abe H, Kubo Y, et al. Expansion of CD4+ CD25+ FoxP3+ regulatory T cells in hepatitis C virus-related chronic hepatitis, cirrhosis and hepatocellular carcinoma. Hepatology Research. 2010;40(2):179-187.
Crossref - Hao C, Zhou Y, He Y, et al. Imbalance of regulatory T cells and T helper type 17 cells in patients with chronic hepatitis C. Immunology. 2014;143(4):531-538.
Crossref - XU HT, Xing TJ, Hao LI, Jun YE. Association of T regulatory cells with natural course and response to treatment with interferon-α in patients with chronic hepatitis B infection. Chin Med J. 2012;125(8):1465-1468.
- Barjon C, Dahlqvist G, Calmus Y, Conti F. Role of regulatory T-cells during hepatitis C infection: From the acute phase to post-transplantation recurrence. Dig Liver Dis. 2015;47(11):913-917.
Crossref - Claassen MA, de Knegt RJ, Tilanus HW, Janssen HL, Boonstra A. Abundant numbers of regulatory T cells localize to the liver of chronic hepatitis C infected patients and limit the extent of fibrosis. J Hepatol. 2010;52(3):315-321.
Crossref - Chang Q, Wang YK, Zhao Q, Wang CZ, Hu YZ, Wu BY. Th17 cells are increased with severity of liver inflammation in patients with chronic hepatitis C. J Gastroenterol Hepatol. 2012; 27(2): 273-278.
Crossref - Balanescu P, Ladaru AN, Voiosu T, Nicolau AD, Ene MI, Balanescu EU. Th17 and IL-17 immunity in chronic hepatitis C infection. Rom J Intern Med. 2012;50(1):13-8.
- Yang C, Cui F, Chen LM, Gong XY, Qin B. Correlation between Th17 and nTreg cell frequencies and the stages of progression in chronic hepatitis B. Mol Med Rep. 2016;13(1):853-859.
Crossref - Zhang JY, Zhang Z, Lin F, et al. Interleukin-17-producing CD4+ T cells increase with severity of liver damage in patients with chronic hepatitis B. Hepatology. 2010;51(1):81-91.
Crossref - Li J, Qiu SJ, She WM, et al. Significance of the balance between regulatory T (Treg) and T helper 17 (Th17) cells during hepatitis B virus related liver fibrosis. PloS one. 2012;7(6):e39307.
Crossref - Su ZJ, Yu XP, Guo RY, et al. Changes in the balance between Treg and Th17 cells in patients with chronic hepatitis B. Diagn Microbiol Infect Dis. 2013;76(4):437-444.
Crossref - Feng H, Yin J, Han YP, et al. Regulatory T cells and IL-17(+) T helper cells enhanced in patients with chronic hepatitis B virus infection. Int J Clin Exp Med. 2015;8:8674-85.
- Collison LW, Workman CJ, Kuo TT, et al. The inhibitory cytokine IL-35 contributes to regulatory T-cell function. Nature. 2007;450(7169):566-569.
Crossref - Teng DK, Liu Y, Lv YF, et al. Elevated interleukin-35 suppresses liver inflammation by regulation of T helper 17 cells in acute hepatitis B virus infection. Int Immunopharmacol. 2019;70:252-259.
Crossref
© The Author(s) 2020. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.