

ISSN: 0973-7510
E-ISSN: 2581-690X
The human pathogen Helicobacter pylori infects around 50% of the global population. Significant proportion of infected individuals with H. pylori can undergo gastritis or gastric adenocarcinoma. The major source and reservoir of infection and transmission with H. pylori is not fully understood, yet. Oral cavity has been proposed to be a reservoir for H. pylori and possibly a major source of gastric reinfection; however, the results are still controversial. In this study a total of sixty Jordanian individuals were tested for the presence of H. pylori in their dental plaques. Samples were analyzed by PCR to detect for the presence of H. pylori using specific primers for H. pylori 16s ribosomal RNA gene. Our data show that all individuals tested in this study were found positive for H. pylori. Although, individuals tested in this study were heterogeneous in term of age, sex, education, and geographical region but this did not influence the presence of H. pylori in the dental plaque of Jordanians. The results of the present study suggest that the oral reinfection route of transmission of H. pylori should be taken into consideration because it may explain the high prevalence of H. pylori associated gastritis in Jordanian people.
DNA: deoxyribonucleic acid, MALT: Mucosa associated lymphoid tissue lymphoma, PCR: polymerase chain reaction, bp: base pair.
Helicobacter pylori is a Gram negative spiral-shaped, microaerophilic bacterium.1,2 H. pylori infection is a major factor in the development of chronic gastritis, gastric and duodenal ulcers.3,4 H. pylori is classified as a Group one Carcinogen based on the world health organization because it is associated with gastric cancer and mucosa associated lymphoid tissue (MALT) lymphoma.5,6 Therefore, it has been suggested that the proper eradication of H. pylori is an important tool for a successful treatment of many H. pylori related diseases.2,7,8 The risk of H. pylori infection is associated with several factors including the age, hygienic conditions, geographical region, and socioeconomic status.9 It is estimated that 50% human population are infected with H. pylori (25-40% in developed and almost 100% in developing countries).10,11 Despite the high prevalence of H. pylori in the stomachs of the world’s population, the mode of transmission is not yet completely known.12 Evidences for the possible route of H. pylori infection are including oral-oral and fecal-oral are provided, but the predominant route of infection has not been proved.13 About 30 years ago, H. pylori was successfully isolated and cultured from the human stomach.14 H. pylori was then isolated from extra-gastric regions such as tonsillar and adenoid tissues,2 saliva, feces, vomitus15 and dental plaque.16
Dental plaque is a biofilm of bacterial growth on the surfaces within the mouth.17 Plaque is associated with oral diseases such as cavities and periodontal diseases and its formation is inevitable process. Bacteria utilize biofilms as a barrier to protect themselves from the attack of the host immune response and from the effect of antibiotics.18 H. pylori is considered a component of the dental plaque which contains more than 600 different microorganisms.13,19-22 However, several studies have concluded that the oral cavity might be the primary reservoir of H. pylori infection. These findings are still controversial, and the exact route and source of H. pylori infection remains elusive.15 H. pylori isolation and culture from the oral cavity is difficult due to the limitation of the use of microaerophilic condition, the long incubation period, the over growth of other oral bacteria, and the inhibitory effect of the oral cavity bacteria on H. pylori. Therefore, polymerase chain reaction (PCR) has been utilized as a reliable tool to detect H. pylori to overcome the difficulties of isolating and culturing H. pylori from the oral biofilm.23,24 Nowadays, PCR is considered an acceptable method for H. Pylori diagnosis and detection form oral cavity samples.21 Different genes can be utilized to screen for H. pylori form oral cavity using PCR; including urease, the 16S ribosomal RNA, and the adhesion genes.25,26 The prevalence of H. pylori in the oral cavities in subjects has not yet been investigated in Jordan. In this study, we aimed to determine the prevalence of H. pylori in oral biofilms among Jordanian volunteers to better understand the correlation of H. pylori transmission to explain the high percentage of H. pylori associated gastric disease in Jordan.27
Study population
A total of 60 dental plaque samples were collected from Jordanian individuals who attended outpatient dental clinic at the medical center of Mutah University. Thirty samples out of 60 were collected from students and the remaining samples were collected from employees working at Mutah University and other visitors. The study population comprised individuals aged 18-52 years. All subjects were interviewed by a questionnaire for socioeconomic and health information. The selection criteria for the sixty volunteers excluded smokers and those who were under antibiotics treatment during the previous four weeks of the sample collection. All volunteers showed good oral hygiene and no oral ulcers. Individuals were asked for the frequency of teeth brushing which was ranging from none to three times daily. Samples were collected after signing an informed consent from all participants of this study which was approved from the scientific research ethical committee in the faculty of medicine at Mutah University.
Dental plaque sample collection
Samples were collected from the surface of teeth with sterile curettes28 from all participants who did not brush their teeth one morning before the samples collection. The collected samples were transferred into 1.5 ml sterile Eppendorf tubes containing 1ml sterile physiological saline solution. Samples were stored at -20p C until tested.
DNA extraction
Genomic deoxyribonucleic acid DNA was isolated and purified using extraction mini kit (OMEGA, Bio-TEK) according to the manufacturer’s instructions. Briefly, samples were thawed then centrifuged at 12,000rpm for 2 min at room temperature to precipitate the dental plaque materials. Supernatants were discarded and the genomic DNA was isolated from the sediments according to the manufacturer’s instructions. DNA was eluted in 100 ìl nuclease free water, quantified on a UV-Nano spectrophotometer (Quawell Technology Inc, USA), and stored at -20°C until tested. Genomic DNA from H. pylori (P12 strain) was used as a positive control.
PCR primers and amplification
The bacterial 16s ribosomal RNA gene was used as a target gene for amplification to detect the presence of H. pylori using PCR. Forward primer 5’-GAAGATAATGACGGTATCTAAC-3 and the reverse primer 5-ATTTCACACCTGACTGACTAT-3’ were used to amplify a 16s ribosomal RNA segment of 150bp (figure 1). Each amplification reaction was performed using Applied Biosystems thermal cycler in a volume of 50 ìl containing 40ng of the extracted DNA and 1 ìl of each primer with a final concentration of 10 pmol. The amplification cycling consisted of initial denaturation at 98p C for 30 sec then by 40 cycles as follow: denaturation at 98p C for 7sec, annealing at57p C for 30 sec, and extension at 72p C for 30 sec. The ûnal DNA extension cycle was performed at 72p C for 7 min. H. pylori DNA positive control was used as in each PCR reaction. All amplification products were analyzed by agarose gel electrophoresis, and the DNA bands were then visualized using Thermo Fischer Scientific gel documentation system.
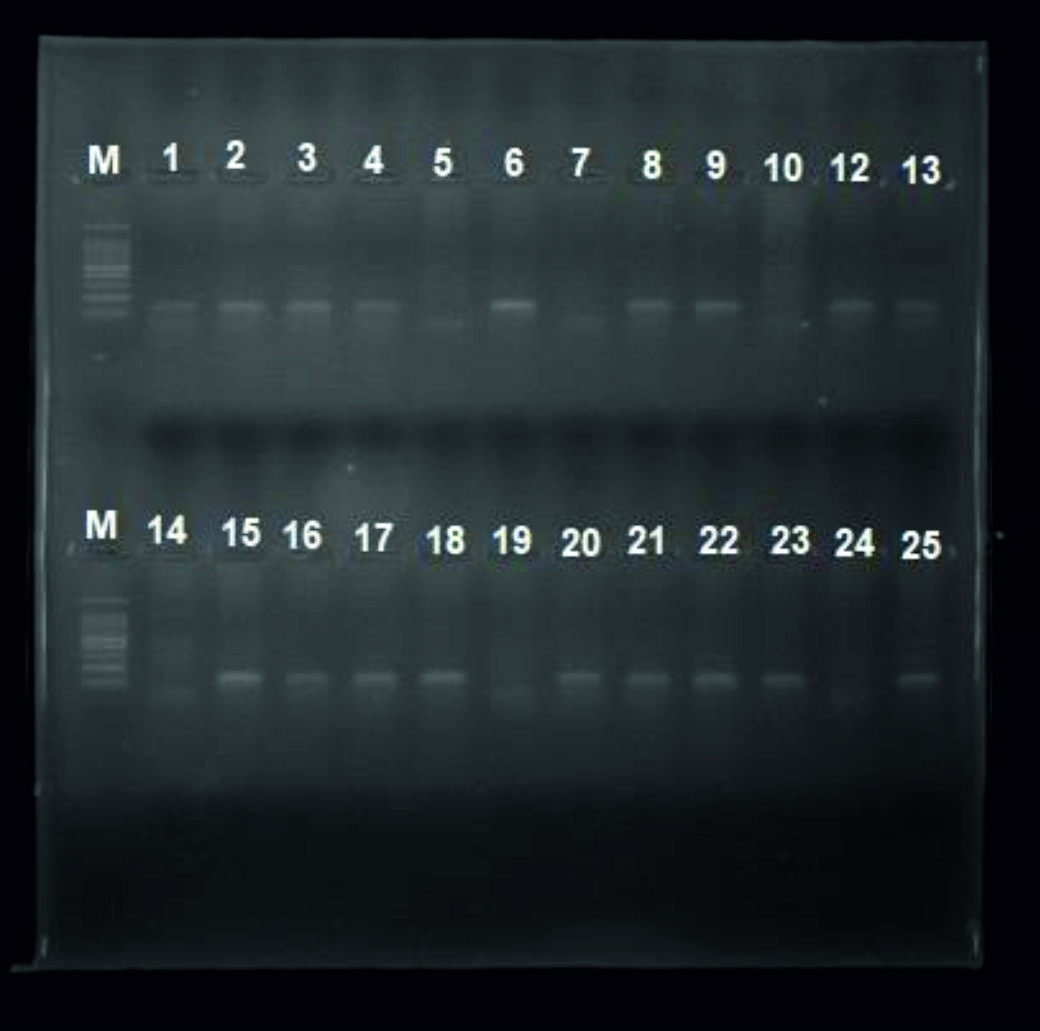
Fig. 1. PCR products gel electrophoresis for the detection of H. pylori in the dental plaque samples. L: 50 bp DNA ladder, lane 1: positive control, lane 2: negative control, lanes 3 to 6: random samples from some participants. PCR: polymerase chain reaction, L: Marker, bp: base pair
In this cross sectional study, a total of 60 dental plaque samples were collected from healthy Jordanian participants. The ages of the participants were between 18 and 52 years old with a mean age of 25.95. Forty one samples were males (68.3%) with a mean age of 23.1 years, while 19 samples were females (31.7%) with a mean age of 25.4 years. Samples were collected randomly from the participants taking into consideration the variation in the social, economic, age, sex, occupational, and educational background as well as the hygienic conditions of the volunteers’ teeth. The PCR results showed that all dental plaque samples were positive for H. pylori as shown in table 1.
Table (1):
The frequency of H. pylori in dental plaque samples in Jordanian participants in relation to age and gender.
| Age | Number | Gender | Percent of H. pylori |
|---|---|---|---|
| 15-29 | 30 | M: 20 | 100% |
| F: 10 | |||
| 30-44 | 17 | M: 12 | 100% |
| F: 5 | |||
| 45-60 | 13 | M: 9 | 100% |
H. pylori infection is one of the most common bacterial infections in human. The role of H. pylori infection has been proved in the development of chronic gastritis, peptic ulcer, gastric cancer, and MALT lymphoma. 3,4 Therefore, the proper control of H. pylori infection would reduce the rate of the gastric associated diseases.3 One of the most important control approaches is identifying the mode of transmission3 because the failure in H. pylori treatment has been found to be in part due to reinfection from extragastric sources.12,29 The human stomach was considered to be the only reservoir for H. pylori until pathogen was detected in extragastric sources such as the dental plaque, water, and saliva.6,30,31
Several difficulties limit the specificity and accuracy of H. pylori identification and diagnosis from oral samples using conventional methods such as bacterial culture. Urease assay was considered as a useful tool to test for the presence of H. pylori, however this test is not indicative for H. pylori infection as other bacteria produce urease such as Streptococcus spp., Hemophilius spp. and Actinomyces spp.12 In addition, H. pylori can transform from its normal helical morphology to a coccoid form which cannot be cultured in vitro. This unique life style of H. pylori is very important determinant for the underestimated prevalence of H. pylori among human using the conventional culture methods.32 Based on that, PCR is considered a useful tool for H. pylori diagnosis from the oral cavity as it is highly sensitive compared to the other conventional methods.23,24 Many studies have demonstrated the sensitivity and specificity of PCR for the detection of H. pylori in clinical samples. PCR was able to detect H. pylori in four biopsies that were tested negative using the conventional culture in vitro.33 Further, using PCR confirmed that 15 out of 23 gastric biopsies were positive for H. Pylori compared with only seven samples confirmed positive for H. pylori using the conventional culture techniques.34
In the present study, the molecular prevalence of H. pylori among Jordanian individuals was 100% regardless of age, gender, hygienic parameters, and geographic distribution. In agreement with our data, H. pylori was detected in the dental plaque of 40/40 (100%) asymptomatic Indian volunteers.35 Similar data was found among German patients tested for H. pylori in the oral cavity (97%).31 Other studies showed different prevalence rate in the presence of H. pylori in the dental plaque samples, for example 73% of dyspeptic Pakistani patients were positive for H. pylori28 compared with 65.6% in Polish volunteers36 and 65% in Saudi patients with dyspepsia.37 Lower prevalence rate was found (37.5%) in Venezuelan patients who had chronic gastritis.38 On the contrary, H. pylori was not detected in 52 Sweden patients who had positive culture for H. pylori from gastric biopsies.39 Similarly, H. pylori was not detected from any of the 290 oral samples of non-dyspeptic French population.40 Further, dental plaque samples were analyzed from 43 Brazilian patients with gastric disease and found to be H. pylori negative.41
There is a controversy in the importance of mouth hygienic conditions in the colonization of H. pylori in the buccal cavity. It was found that the occurrence of H. pylori antigens in dental plaque of natural teeth is not associated with oral health status.36 While, others contraindicated that and found the oral health parameters are determinants for the colonization of H. pylori in the dental plaque.42 Some reports suggested that the failure in H. pylori treatment has been linked to be in part to the reinfection from the oral cavity.12,29,38 It has been demonstrated that the dental plaque unaffected by the triple drug therapy of H. pylori which might raise an alarm for the possibility of gastric reinfection from the dental plaque after a successful therapy.43 Therefore, the detection of H. pylori in dental plaque samples is considered a noninvasive procedure compared to the endoscopy method and it might be used as an important tool to monitor the efficiency of treatment of H. pylori associated gastritis.43
Although the prevalence of the H. pylori in dental plaque was shown to be very low in some studies, our current study showed that the prevalence of H. pylori in the dental plaque samples from Jordanian people is unexpectedly high and unexplained. Our data might explain the high prevalence (78%) of H. pylori among Jordanian patients with gastric diseases.27 It is necessary to pay close attention to the dental plaque as a possible reservoir of H. pylori and a possible source of reinfection and infection among Jordanians.
In conclusion, our study proposes the significance of the oral-oral route of H. pylori transmission among Jordanian people due to the 100% prevalence of H. pylori in the selected dental plaque samples which mandates protective measures to prevent the transmission to possibly people with negative dental plaque for H. pylori and to follow new treatment strategies for patients with gastritis and positive for H. pylori in their dental plaques.
ACKNOWLEDGMENTS
The authors deeply appreciate and thank Prof. Dr. Thomas F Meyer- a director at Max Planck Institute for Infection Biology/Berlin- for his support to do the genetic analysis in his lab. Also, the thank extends to the German academic exchange service (DAAD) for their financial support. We would to thank the staff at the dental clinic for helping in samples collection.
- Amiri N, Abiri R, Eyvazi M, Zolfaghari MR, Alvandi A. The frequency of Helicobacter pylori in dental plaque is possibly underestimated. Archives of oral biology 2015; 60: 782-788.
- Payao L, Rasmussen, L. Helicobacter pylori and its reservoirs: A correlation with the gastric infection. World journal of gastrointestinal pharmacology and therapeutics 2016; 7: 126-132.
- Goodman K , Correa P. The transmission of Helicobacter pylori. A critical review of the evidence. International journal of epidemiology 1995; 24: 875-887.
- Graham D, Yamaoka Y. pylori and cagA: relationships with gastric cancer, duodenal ulcer, and reflux esophagitis and its complications. Helicobacter 1998; 3: 145-151.
- Adler I, Muiño A, Aguas S, Harada L, Diaz M et al. Helicobacter pylori and oral pathology: relationship with the gastric infection. World journal of gastroenterology 2014; 20: 9922-9935.
- Al Sayed A, Pradeep S, Kavitha P, Shankargouda K, Preethanath P et al. Oral Cavity as an Extragastric Reservoir of Helicobacter pylori. ISRN gastroenterology 2014, 261369, doi:10.1155/2014/261369 (2014).
- Marshall BJ, Goodwin CS, Warren JR, Murray R, Blincow ED et al. Prospective double-blind trial of duodenal ulcer relapse after eradication of Campylobacter pylori. Lancet 1988; 2:1437-1442.
- Tatsuta M, Iishi H, Yokota Y. Effects of Helicobacter pylori infection on healing and recurrence of gastric ulcers. The American journal of gastroenterology 1995; 90: 406-410.
- Wang A., Peura D. The prevalence and incidence of Helicobacter pylori-associated peptic ulcer disease and upper gastrointestinal bleeding throughout the world. Gastrointestinal endoscopy clinics of North America 2011; 21: 613-635.
- Ali M, Whitehead M. Clearance of chronic psoriasis after eradication therapy for Helicobacter pylori infection. Journal of the European Academy of Dermatology and Venereology : JEADV 2008; 22: 753-754.
- Windsor HM, Abioye-Kuteyi EA, Leber JM, Morrow SD, Bulsara MK et al. Prevalence of Helicobacter pylori in Indigenous Western Australians: comparison between urban and remote rural populations. The Medical journal of Australia 2005; 182: 210-213.
- Glupczynski Y, Burette A. Drug therapy for Helicobacter pylori infection: problems and pitfalls. The American journal of gastroenterology 1990; 85: 1545-1551.
- Garcia A, Salas-Jara M, Herrera C, Gonzalez C. Biofilm and Helicobacter pylori: from environment to human host. World journal of gastroenterology 2014; 20: 5632-5638.
- Marshall B, Warren R. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet 1984; 1: 1311-1315.
- Ahmed KS, Khan AA, Ahmed I, Tiwari SK, Habeeb MA et al. Prevalence study to elucidate the transmission pathways of Helicobacter pylori at oral and gastroduodenal sites of a South Indian population. Singapore medical journal 2006; 47: 291-296.
- Krajden S, Fuksa M, J Anderson J, Kempston J, Boccia A et al. Examination of human stomach biopsies, saliva, and dental plaque for Campylobacter pylori. Journal of clinical microbiology 1989; 27: 1397-1398.
- Socransky S, Haffajee A. Dental biofilms: difficult therapeutic targets. Periodontology 2002;28: 12-55.
- Assumpção MB, Martins LC, Melo Barbosa HP, Barile KA, de Almeida SS et al. Helicobacter pylori in dental plaque and stomach of patients from Northern Brazil. World journal of gastroenterology 2010; 16: 3033-3039.
- Aas J,Griffen A,Dardis S, Lee A, Olsen I et al. Bacteria of dental caries in primary and permanent teeth in children and young adults. Journal of clinical microbiology 2008; 46: 1407-1417.
- Liu, Y. et al. An epidemiologic study on the correlation between oral Helicobacter pylori and gastric H. pylori. Current microbiology 2009; 58; 449-453.
- Lukes P, Astl J, Pavlík E, Potuzníková B, Sterzl I et al. Helicobacter pylori in tonsillar and adenoid tissue and its possible role in oropharyngeal carcinogenesis. Folia biologica 2008; 54: 33-39.
- Silva DG, Stevens RH, Macedo JM, Albano RM, Falabella ME et al. Detection of cytotoxin genotypes of Helicobacter pylori in stomach, saliva and dental plaque. Archives of oral biology 2009; 54: 684-688.
- Czesnikiewicz-Guzik M, Bielanski W, Guzik T, Loster B, Konturek J. Helicobacter pylori in the oral cavity and its implications for gastric infection, periodontal health, immunology and dyspepsia. Journal of physiology and pharmacology : an official journal of the Polish Physiological Society 2005; 56 Suppl 6: 77-89.
- Dowsett S, Kowolik J. Oral Helicobacter pylori: can we stomach it? Critical reviews in oral biology and medicine : an official publication of the American Association of Oral Biologists 2003; 14: 226-233.
- Chong K, Lou Q, Fitzgerald J, Lee C. H. Evaluation of 16S rRNA gene PCR with primers Hp1 and Hp2 for detection of Helicobacter pylori. Journal of clinical microbiology 1996; 34: 2728-2730.
- Watanabe T, Tomita S, Kudo M, Kurokawa M, Orino A et al. Detection of Helicobacter pylori gene by means of immunomagnetic separation-based polymerase chain reaction in feces. Scandinavian journal of gastroenterology 1998; 33: 1140-1143.
- Nimri F, Matalka I., Bani Hani K, Ibrahim M. Helicobacter pylori genotypes identified in gastric biopsy specimens from Jordanian patients. BMC gastroenterology 2006; 6: 27, doi:10.1186/1471-230x-6-27 (2006).
- Chitsazi T, FattahiE, Farahani R, Fattahi, S. Helicobacter pylori in the dental plaque: is it of diagnostic value for gastric infection? Medicina oral, patologia oral y cirugia bucal 2006; 11: E325-328.
- Coelho LG, Passos MC, Chausson Y, Costa EL, Maia AF et al. Duodenal ulcer and eradication of Helicobacter pylori in a developing country. An 18-month follow-up study. Scandinavian journal of gastroenterology 1992; 27: 362-366.
- Ashbolt, N. J. Microbial contamination of drinking water and disease outcomes in developing regions. Toxicology 2004; 198: 229-238.
- Song Q, Lange T, Spahr A, Adler G, Bode G. Characteristic distribution pattern of Helicobacter pylori in dental plaque and saliva detected with nested PCR. Journal of medical microbiology 2000; 49, 349-353.
- Bode G, Mauch F, Malfertheiner P. The coccoid forms of Helicobacter pylori. Criteria for their viability. Epidemiology and infection1993; 111: 483-490.
- Hammar M, Tyszkiewicz T, WadstromT, O’Toole W. Rapid detection of Helicobacter pylori in gastric biopsy material by polymerase chain reaction. Journal of clinical microbiology 1992; 30: 54-58.
- Clayton L, Kleanthous H, Coates P, Morgan D, Tabaqchali S. Sensitive detection of Helicobacter pylori by using polymerase chain reaction. Journal of clinical microbiology 1992; 30: 192-200.
- Majmudar P, Shah M, Dhunjibhoy K, DesaiG. Isolation of Helicobacter pylori from dental plaques in healthy volunteers. Indian journal of gastroenterology : official journal of the Indian Society of Gastroenterology 1990; 9: 271-272.
- Namiot DB1, Leszczyñska K, Namiot Z, Chilewicz M, Bucki R et al. The occurrence of Helicobacter pylori antigens in dental plaque; an association with oral health status and oral hygiene practices. Advances in medical sciences 2010; 55: 167-171.
- Al Asqah M, Al Hamoudi N, Anil S, Al Jebreen A, Al-Hamoudi K. Is the presence of Helicobacter pylori in dental plaque of patients with chronic periodontitis a risk factor for gastric infection? Canadian journal of gastroenterology = Journal canadien de gastroenterologie 2009; 23: 177-179.
- Berroteran A, Perrone M, Correnti M, Cavazza ME, Tombazzi C et al. Detection of Helicobacter pylori DNA in the oral cavity and gastroduodenal system of a Venezuelan population. Journal of medical microbiology 2002; 51: 764-770.
- Bernander S, Dalén J, Gästrin B, Hedenborg L, Lamke LO et al. Absence of Helicobacter pylori in dental plaques in Helicobacter pylori positive dyspeptic patients. European journal of clinical microbiology & infectious diseases : official publication of the European Society of Clinical Microbiology 1993; 12: 282-285.
- Martinez-Gomis J, Diouf A, Lakhssassi N, Sixou M. Absence of Helicobacter pylori in the oral cavity of 10 non-dyspeptic subjects demonstrated by real-time polymerase chain reaction. Oral microbiology and immunology 2006; 21: 407-410.
- Silva Rossi-Aguiar VP, Navarro-Rodriguez T, Mattar R, Siqueira de Melo Peres MP, Correa Barbuti R et al. Oral cavity is not a reservoir for Helicobacter pylori in infected patients with functional dyspepsia. Oral microbiology and immunology 2009; 24: 255-259.
- Silva DG, Stevens RH, Macedo JM, Albano RM, Falabella ME et al. Presence of Helicobacter pylori in supragingival dental plaque of individuals with periodontal disease and upper gastric diseases. Archives of oral biology 2010; 55: 896-901.
- Desai G, Gill H, Shankaran K, Mehta, P, Prabhu R. Dental plaque: a permanent reservoir of Helicobacter pylori? Scandinavian journal of gastroenterology 1991; 26: 1205-1208.
© The Author(s) 2017. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.