


ISSN: 0973-7510
E-ISSN: 2581-690X
The emergence and spread of carbapenem-resistant Gram-negative bacteria is a worldwide emerging public health threat responsible for large number of nosocomail infections. Metallo-b-lactamases including IMP, VIM, and NDM as well as carbapenem hydrolyzing class D b-lactamase (OXA-48 like) are the predominant types that confer resistance to Carbapenem group of antibiotics. The aim of this study was to identify the carbapenemase encoding genes among Gram negative bacteria isolates. 42 isolates were identified depending on routine morphological tests followed by species identification using the VITEK 2 system. The 16S rDNA gene sequence was used for confirmation of the detection of Enterobacteriaceae and Pseudomonas aeruginosa. Antimicrobial susceptibility testing was performed using VITEK 2 system. For phenotypic detection of carbapenemase activity, modified carbapenem inactivation method (mCIM) was performed. The carbapenemases encoding genes (blaIMP, blaSPM, blaVIM, blaNDM, blaKPC, blaBIC, blaOXA, blaAIM, blaSIM, blaGIM, blaDIM) were amplified by PCR and the amplified products were sequenced. Forty two Gram-negative bacteria isolates including 25 of P. aeruginosa (59.5%) and 17 of Enterobacteriaceae family (40.4%) were identified. According to PCR-based method results, carbapenemase gene blaOXA-48 was detected in 31(73.8%) of isolates, blaVIM in 23 (54.7%) and blaNDM in 2(4.76%) of isolates. Twelve (28.5%) of isolates harbored a combination of blaOXA-48 and blaVIM, (2.4%) coexistence blaOXA-48 and blaNDM gene and (2.4%) of isolates harbored a blaOXA-48, blaVIM and blaNDM genes. No other carbapenemase genes were identified. Based on the present study, it was concluded that the high prevalence was in blaOXA-48 gene, followed by blaVIM gene among carbapenemase-producing Gram-negative bacteria isolates.
Enterobacteriaceae Pseudomonas aeruginosa, Carbapenemases.
Gram-negative bacteria that produce Carbapenemase have been related to increased mortality and critical nosocomial outbreaks that represent the main challenge in both therapeutic and infection control1.
The concern of carbapenemase-producing Gram-negative bacteria that emerged currently is due to it is often related to the occurrence of multiple drug resistant isolates for which few choices of antimicrobials stay available2.
Carbapenems are b-lactam antibiotics that used most frequently as last resource antibiotics for treating of multidrug-resistant Gram negative bacilli-causing infections, since they have the wide spectrum of bactericidal action and their stability against most of the b-lactamases, including ESBLs3.
The increase of carbapenem resistance in these microorganisms is a major concern globally. The most common mechanism of resistance is the production of carbapenem-hydrolysing enzymes, carbapenemases that hydrolyse most b-lactams4.
These enzymes encoding by multiple genes of resistance, which is associated with different mobile genetic determinants, thus conferring resistance to various classes of antimicrobials, such as aminoglycosides, fluoro-quinolones, tetracyclines, trimethoprim, sulphonamides, and phenicols5.
The major public health threat is with transmissible carbapenemases, which can increase the rate of mortality and limit the choice of appropriate antibiotic therapy6. The transmissible enzymes can be acquired unpredictably by important nosocomial pathogens such as Pseudomonas aeruginosa, Acinetobacter baumannii and members of the family Enterobacteriaceae7.
The most serious form of carbapenem resistance is mediated by carbapenem-hydrolyzing b-lactamases, including metallo-b-lactamases (MBLs), such as imipenemase (IMP), Verona imipenemase (VIM), New Delhi metallo-b-lactamase (NDM), Ambler class A Klebsiella pneumoniae carbapenemase (KPC), and class D oxacillinase-48 (OXA-48)8.
Because of the lack of implementing standardized protocols for detection of carbapenemase-producing isolates in many countries that probable to be the major reservoirs, the actual prevalence of these producers is still unknown. It is estimated that we are on the rim of a global epidemic with carbapenemase-producing isolates, which in the hospital environment is likely to be caused mostly by all types of nosocomial carbapenemase-producers (e.g. KPC, IMP, VIM, NDM and OXA-48)9.
In Iraq, we showed that a significant increase in carbapenem-resistant bacteria in the last two decades, especially after the 2003 War, maybe is due to the Iraq’s openness to the world and the entry of foreign workers, especially from the endemic area from the Indian subcontinent like Bangladesh and other countries.
For all of the mentioned above, as well as, few report investigated the molecular basis of resistance to carbapenems among Gram-negative bacteria, this study aimed to identify the genes which is responsible for encoding carbapenemase enzymes in these organisms.
Bacterial isolates
A total of 42 different Gram-negative isolates were collected from various patient specimens from different hospitals in Baghdad city, Iraq during a period between October 2017 and February 2018. The isolates were identified initially depending on morphological characteristics as described previously10, followed by identification by using VITEK® 2 compact system (bioMeriux, France). Genotypic method was used to confirm the identification of isolates at species level using 16S rDNA gene sequences.
Antimicrobial susceptibility test
Antimicrobial susceptibility test was performed with the VITEK 2 system (bioMe´rieux, France) using AST 69 card as described by the manufacturer. The tested antibiotics were: Ampicillin, Amoxicillin/Clavulanic Acid, Ampicillin / Sulbactam, Cefazolin, Ceftazidime, Ceftriaxone, Cefepime, Ciprofloxacin, Levofloxacin, Imipenem, Amikacin, Gentamicin, Trimethoprim/Sulfamethoxazole and Nitro-furantoin.
Phenotypic detection of carbapenemase production
The modified carbapenem inactivation method (mCIM) was performed according to CLSI guidelines11. In briefly, using sterile inoculating loop, 1µl of test organism was suspended in 2ml of tryptic soy broth, the bacterial suspension was homogenized by vortex. Then, a 10-µg meropenem disk was immersed into the suspension. Subsequently, the culture was incubated for 4 hours at 35°C, prepared 0.5 McFarland suspension of E. coli ATCC® 25922(a carbapenem-susceptible strain) that was inoculated on Muellar-Hinton agar(MHA) plates streaked as cell lawn.
After the incubation, the disk was removed using a 10-µl inoculating loop; the loop was dragged along the edge of the tube during removal to remove excess liquid, and the disk was placed onto the inoculated MHA plate, which was then incubated in for 18-24 hours at 35°C. Following the incubation, diameter of the inhibition zone around the disc was measured, a zone diameter of 6-10 mm or presence of colonies within a 16–18 mm zone was considered to be a positive result, 16–18 mm an indeterminate result, and 19 mm a negative result.
Genotypic identification of carbapenemase-encoding genes
DNA isolation of bacteria
Pure culture of bacterial isolates were grown overnight in liquid nutrient broth medium (NB) for the isolation of genomic DNA using the Genomic DNA purification kit (Promega, USA) according to the manufacturers protocol.
All isolates were subjected to molecular screening to detect carbapenemase-encoding genes by using PCR amplification technique. In this study, multiplex PCR was used to detect carbapenemase encoding genes from clinical isolates and the PCR products were sequenced.
Multiplex PCR
Eleven pairs of primers (Alpha DNA, Canada) were used in this method, that defined into 3 multiplex reaction. No.1 included detection of blaIMP, blaSPM and blaVIM genes, No.2 included detection of blaNDM, blaKPC, blaBIC and blaOXA genes and No. 3 included detection of blaAIM, blaSIM, blaGIM and blaDIM genes.
Different primers (Table 2) were used, the PCR reaction mixture contained: 2µl of template DNA, 12.5µl of Go Taq Green Master Mix (2x) (Promega (USA), 1µl from each of the following primers : IMP, SPM ,VIM, NDM, BIC, KPC or OXA and the volume was completed to 25µl with nuclease free water. While the reaction mixture of 25µl for each of the following primers: AIM, SIM, GIM or DIM composed from 2µl of template DNA,12.5µl of Go Taq Green Master Mix, 1µl of each primers and 1.5µl of dimethyl sulfoxide (DMSO) and the volume was completed to 25µl with nuclease free water12. Cycle conditions were as followed: 10 min at 94°C and 36 cycles of amplification consisting of 30 sec at 94°C, 40 sec at 52°C and 50 sec at 72°C, with 5 min at 72°C for the final extension.
The amplified products were electrophoresed in 2% agarose gel in 1x TBE buffer containing red safe dye at 100 V for 50 minutes. Then, the PCR products were visualized under UV light by UV transilluminator. The E.coli ATCC 25922 strain was used as negative control.
Sequencing of PCR products
The amplified PCR products were sequenced at Macrogen DNA sequencing Company (Seoul, Korea). DNA sequences were analyzed and compared with standard strain using BLAST (Basic Local Alignment Search Tool) in National Center for Biotechnology Information website (http://www.ncbi.nlm.nih.gov/ BLAST).
Genebank accession numbers
The 16S rDNA gene, blaVIM-2 gene, blaOXA-48 gene and blaNDM gene sequences from this study were deposited in Genbank database under accession numbers MK182251 to MK182258, MK156197 to MK156202 and MK159338 to MK159352.
Forty two clinical isolates of Gram-negative bacteria (Pseudomonas aeruginosa and members of Enterobacteriaceae family) were isolated from 32 patients including: 40 (95.2%) isolates from burns and 2 (4.76%) isolates from urine infection were collected. From 42 isolates, 25(59%) were P. aeruginosa and 17(40%) were Enterobacteriaceae (six of Klebsiella pneumoniae, seven of E. coli and four of Enterobacter cloacae) (Table 2).
Table (2):
Distribution of carbapenemases encoding genes among isolates
Isolates No. |
Bacterial species |
Genes |
Isolation source |
|---|---|---|---|
SN1 |
Escherichia coli |
blaVIM |
Burn |
SN2 |
Enterobacter cloacae |
blaVIM |
Burn |
SN3 |
Pseudomonas aeruginosa |
blaVIM |
Burn |
SN4 |
Escherichia coli |
blaVIM |
Burn |
SN5 |
Pseudomonas aeruginosa |
blaVIM& blaOXA-48 |
Burn |
SN6 |
Pseudomonas aeruginosa |
blaVIM& blaOXA-48 |
Burn |
SN7 |
Pseudomonas aeruginosa |
blaVIM&blaNDM& blaOXA-48 |
Burn |
SN8 |
Pseudomonas aeruginosa |
blaVIM&blaOXA-48 |
Burn |
SN9 |
Pseudomonas aeruginosa |
blaVIM |
Burn |
SN10 |
Pseudomonas aeruginosa |
blaNDM& blaOXA-48 |
Burn |
SN11 |
Pseudomonas aeruginosa |
blaVIM&blaOXA-48 |
Burn |
SN12 |
Pseudomonas aeruginosa |
blaOXA-48 |
Burn |
SN13 |
Pseudomonas aeruginosa |
blaVIM |
Burn |
SN14 |
Pseudomonas aeruginosa |
blaVIM |
Burn |
SN15 |
Pseudomonas aeruginosa |
blaVIM& blaOXA-48 |
Burn |
SN16 |
Escherichia coli |
blaVIM |
Burn |
SN17 |
Pseudomonas aeruginosa |
blaOXA-48 |
Burn |
SN18 |
Enterobacter cloacae |
blaVIM&blaOXA-48 |
Burn |
SN19 |
Pseudomonas aeruginosa |
blaOXA-48 |
Burn |
SN20 |
Pseudomonas aeruginosa |
blaOXA-48 |
Burn |
SN21 |
Pseudomonas aeruginosa |
blaVIM |
Burn |
SN22 |
Pseudomonas aeruginosa |
None |
Burn |
SN23 |
Pseudomonas aeruginosa |
blaOXA-48 |
Burn |
SN24 |
Pseudomonas aeruginosa |
blaOXA-48 |
Burn |
SN25 |
Pseudomonas aeruginosa |
blaOXA-48 |
Burn |
SN26 |
Escherichia coli |
blaOXA-48 |
Burn |
SN27 |
Escherichia coli |
blaVIM& blaOXA-48 |
Burn |
SN28 |
Klebsiellapneumoniae |
blaOXA-48 |
Burn |
SN29 |
Pseudomonas aeruginosa |
blaOXA-48 |
Burn |
SN30 |
Escherichia coli |
blaVIM |
urine |
SN31 |
Klebsiellapneumoniae |
blaOXA-48 |
Burn |
SN32 |
Enterobacter cloacae |
blaOXA-48 |
Burn |
SN33 |
Pseudomonas aeruginosa |
blaVIM& blaOXA-48 |
Burn |
SN34 |
Enterobacter cloacae |
blaOXA-48 |
urine |
SN35 |
Klebsiellapneumoniae |
blaVIM& blaOXA-48 |
Burn |
SN36 |
Klebsiellapneumoniae |
blaOXA-48 |
Burn |
SN37 |
Pseudomonas aeruginosa |
blaOXA-48 |
Burn |
SN38 |
Klebsiellapneumoniae |
blaOXA-48 |
Burn |
SN39 |
Pseudomonas aeruginosa |
blaVIM&blaOXA-48 |
Burn |
SN40 |
Klebsiellapneumoniae |
blaVIM&blaOXA-48 |
Burn |
SN41 |
Escherichia coli |
blaOXA-48 |
Burn |
SN41 |
Pseudomonas aeruginosa |
blaVIM& blaOXA-48 |
Burn |
The patterns of antimicrobial resistance were as followed: (100%) to ampicillin and cefazolin and Ceftriaxone, (95.2%) to ampicillin/sulbactam and imipenem, (92.8%) to amoxicillin/clavulanic acid and trimethoprim/sulfametho-xazol, (85.71%) to cefepime, (80.95%) to ceftazidime and gentamicin, (76.1%) to amikacin, (69.04%) to ciprofloxacin, (66.6%) to levofloxacin and (64.28%) to nitrofurantoin (Fig. 1).
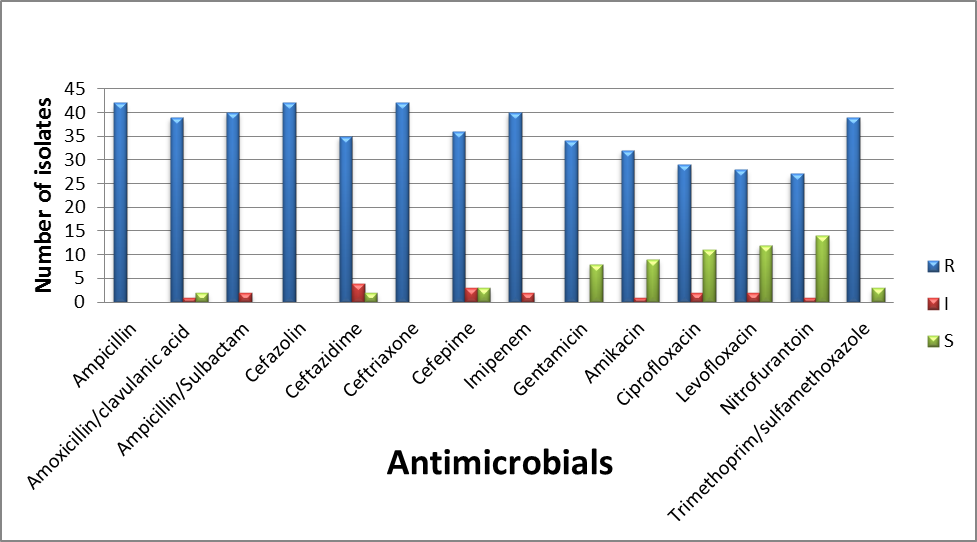
Fig. 1. The Antibiogram pattern of isolates towards antimicrobials used in this study. (R): Resistant,
(I): Intermediate and (S): Susceptible.
For mCIM, all isolates showed positive results (25 isolates of Pseudomonas aeruginosa and 17 isolates of Enterobacteriaceae family) indicating the production of carbapenemase by these strains. Molecular tests confirmed that at least one carbapenemase gene in all isolates that were phenotypically carbapenemase positive, with the exception of one Pseudomonas aeruginosa isolate was carbapenemase-positive by phenotypic test despite being negative for the detection of carbapenemase encoding genes.
Multiplex PCR-based methods were conducted to detect the carbapenem-resistant genes. The most prevalent carbapenemase gene blaOXA-48 was found in 31(73.8%) of the 42 isolates, followed by blaVIM gene that was detected in 23 (54.7%) and blaNDM gene in 2(4.76%). The results showed the presence of blaOXA-48 gene were found in 19(45.2%) of P. aeruginosa, 6 (14.2%) of K.pneumoniae, 3(7.1%) of E.coli isolates and in 3(7.1%) of E. cloacae; blaVIM gene in 14(33.3%) of P.aeruginosa isolates, 2(4.7%) of K.pneumoniae isolates, 5(11.9%) of E.coli isolates and 2(4.7%) of E. cloacae isolates and presence of blaNDM gene in 2(4.76%) of P.aeruginosa (Table 1). On the other hand, blaIMP, blaSPM, blaKPC, blaBIC, blaAIM, blaSIM, blaGIM and blaDIM genes were not detected in all isolates.
Table (1):
The primers used in this study
| Gene | Primer | Sequence (5′- 3′) | Product size | Reference |
|---|---|---|---|---|
| PASS | PA-SS-F | GGGGGATCTTCGGACCTCA | 956 | 13 |
| PA-SS-R | TCCTTAGAGTGCCCACCCG | |||
| 16SrRNA | 27 F | AGAGTTTGATCCTGGCTCAG | 1183 | 14 |
| 1492 R | CTTGTGCGGGCCCCCGTCAATTC | |||
| blaIMP | IMP-F | GGAATAGAGTGGCTTAAYTCTC | 232 | 12 |
| IMP-R | GGTTTAAYAAAACAACCACC | |||
| blaSPM | SPM-F | AAAATCTGGGTACGCAAACG | 271 | |
| SPM-R | ACATTATCCGCTGGAACAGG | |||
| bla AIM | AIM-F | CTGAAGGTGTACGGAAACAC | 322 | |
| AIM-R | GTTCGGCCACCTCGAATTG | |||
| blaVIM | VIM-F | GATGGTGTTTGGTCGCATA | 390 | |
| VIM-R | CGAATGCGCAGCACCAG | |||
| blaOXA | OXA-F | GCGTGGTTAAGGATGAACAC | 438 | |
| OXA-R | CATCAAGTTCAACCCAACCG | |||
| blaGIM | GIM-F | TCGACACACCTTGGTCTGAA | 477 | |
| GIM-R | AACTTCCAACTTTGCCATGC | |||
| blaBIC | BIC-F | TATGCAGCTCCTTTAAGGGC | 537 | |
| BIC-R | TCATTGGCGGTGCCGTACAC | |||
| blaSIM | SIM-F | TACAAGGGATTCGGCATCG | 570 | |
| SIM-R | TAATGGCCTGTTCCCATGTG | |||
| blaNDM | NDM-F | GGTTTGGCGATCTGGTTTTC | 621 | |
| NDM-R | CGGAATGGCTCATCACGATC | |||
| blaDIM | DIM-F | GCTTGTCTTCGCTTGCTAACG | 699 | |
| DIM-R | CGTTCGGCTGGATTGATTTG | |||
| blaKPC | KPC-Fm | CGTCTAGTTCTGCTGTCTTG | 798 | |
| KPC-Rm | CTTGTCATCCTTGTTAGGCG | |||
| Pre NDM | pre-NDM-F | CACCTCATGTTTGAATTCGCC | 984 | 15 |
| pre- NDM-R | CTCTGTCACATCGAAATCGC | |||
Interestingly, twelve isolates (28.5%) harbored a combination of blaOXA-48 and blaVIM, one isolate (2.4%) co-harboring three carbapenemase-encoding genes blaOXA-48 and blaNDM gene and 1(2.4%) harboring blaOXA-48, blaVIM and blaNDM genes.
Carbapenemase-producing bacteria have become a major problem worldwide, which has emerged due to the increased dependence on carbapenems as a last resource to treat bacteria with multidrug-resistant16.
Carbapenemases represent the stringent threat for global human health and stand as one of the most challenging issues facing infectious disease containment in the subsequent years17.
Notwithstanding the small number of isolates, the author found the dominant OXA-48 carbapenemases among studied isolates.
The most current and concern development is the rapid rise in emerging and dissemination of OXA-48, particularly in K. pneumoniae. In 2001, the OXA-48-producing Enterobacteriaceae was first identified in Turkey, then later reported in various countries including the Middle East, North Africa, and Europe18.
In a local study carried by Abdulla et al. (2016), they reported that the blaOXA-48 genes were detected in 25%, of the E.coli isolates and 21.4% in K. pneumoniae isolates19.
Several studies in regional countries reported the predominance of blaOXA-48 among Gram negative bacteria, as it was 49% in Arabian Gulf 20, 53.3% in the UAE21, 88% in Lebanon22, 49.2% in Egypt 16 and 86% in Turkey 8, on the other hand, a study by Mohamed et al., reported decrease in the rate (22.4%) of this gene in P.aeruginosa isolates23.
The increasing incidence of blaOXA-48 has been described in varying worldwide countries, in France, blaOXA-48 gene represented 76.8% of carbapenemase producing K. pneumoniae, 81.1% of carbapenemase- producing E.coli, 75.8% of carbapenemase-producing Enterobacter spp.24, in Romania, 80% of K.pneumonie isolates harbored a blaOXA-48 gene25, while in Canada, Mataseje et al., reported that blaOXA-48 found in 31.3% of isolates 26.
In regard to existence of the blaVIM gene, the results also showed increasing in prevalence rate, as it was 54.7% of carbapenem-resistant isolates have possessed this gene.
A local study done by Al-Jubori et al, (2016) showed that the prevalence rate of blaVIM gene was 25% in A. baumannii27, while another study done by Hammadi et al .(2015), reported that all E.coli isolates did not carry blaVIM gene 28.
The VIM types are the most frequent among class B carbapenemases which have been detected in all continents29. VIM enzymes were firstly reported in isolates of P. aeruginosa, and then emerged in Enterobacteriaceae as well. Subsequently in a number of regional countries, a study carried out in Saudi Arabia describing that P.aeruginosa strain harboring the blaVIM-2 gene from a Saudi patient hospitalized in France 30.
In Iran, Rajabnia et al. (2015), reported that the blaVIM-1 gene are presence in 30% of K. pneumoniae isolates 31, while in Turkey, Haciseyitoglu et al. (2017) found that the percentage rate of this gene was low when it reached only 10% in E.cloacae32.
Hammami et al. (2011) revealed that the percentage of blaVIM-2 gene was 67% in Tunisia33.
In Romania, Mereuta et al. (2013), showed that 48% of P.aeruginosa isolates carried ablaVIM-2 gene34, while in Korea, Hong et al. showed that 69% of isolates harbored the blaVIM-2 gene35, on the other hand, Touati et al. (2013) mentioned that the percentage rate was 82% of the studied isolates36.
Since the detection of NDM-1 is firstly reported in India, there has been a global rise in the dissemination of NDM-1 carrying organisms. At first, the existence of NDM-1 was predominantly reported in Enterobacteriaceae, but reports occurring recently pointed out to its spread in Acinetobacter spp. and Pseudomonas spp. as well37.
The author found that blaNDM gene is presence in two isolates (4.7%) of P.aeruginosa among carbapenem resistant isolates.
In local studies, Al-shara et al.(2014) reported that out of 36 carbapenem resistant P.aeruginosa isolates, only 5.6% of isolates harbored blaNDM gene 38, another study by AL-Harmoosh (2015) showed that the prevalence rate of blaNDM-1 gene was 20%39, while in recent study by Hussein (2017), revealed that blaNDM-1 gene was 40% in E.coli isolates40, however Hammoudi et al. showed that the percentage of the prevalence of blaNDM-1 gene was 100% in isolates41.
Bacterial isolates that produce NDM-1 enzyme may express numerous other unrelated resistance genes, such as OXA-48 type and VIM type that encode other carbapenemases, AmpC, extended-spectrum beta-lactamases, and other classes of antimicrobials42.
The prevalence of NDM-1 producing isolates were reported from different countries including the Gulf Corporation Council (GCC) which investigated in a total of 200 isolates collected from 16 hospitals in Saudi Arabia, Kuwait, Oman and the United Arab Emirates. Overall, NDM-1 was the most common encountered carbapenemase gene 46.5%43, 47.6% in Egypt16, 29.5% in Turkey8 and 7.8% in Tunisia44.
In Bangladesh, Khatun et al. (2015), reported the rate 73.7% of blaNDM-145, in Romania a study done by Dortet et al.(2015), revealed that 15 carbapenemase producing Enterobacteriaceae, were recovered from patients hospitalized between 2011 and 2013, 60% harbored a blaNDM-1 gene25, 100% in Russia46, as well as Dort et al. (2013) reported that the percentage of blaNDM-1 gene was 7.9% in France24.
The global emergence of double- and multi-carbapenemase-producing hospital-acquired Gram-negative pathogens, are mostly Klebsiella pneumoniae, Pseudomonas aeruginosa, and Acinetobacter baumannii47.
In Kuwait, Jamal et al. reported that two of the blaNDM-1-producing isolates co-harbored blaOXA-48 carbapenemase48, 22.1% in Dubai21, 4.5% in Turkey32 and 92.1% in Tunis44, while in India, kaziet al.(2014) revealed that 3.6 %of the isolates possessed dual carbapene-maseblaNDM and blaVIM genes37.
A K. pneumoniae co-producing NDM-1 and OXA-232 (an OXA-48 variant) was imported to the USA from India49, and another was found also in a French hospital50, where its cross-transmission was documented47.
The ratio of carbapenemase producing isolates differs by geographic region, type of infection, specimen source, and selective pressure due to antibiotics. This difference also associated with variation among the different patients studied and the different rates of antibiotic used in different hospitals51.
The diversity of carbapenemases depends on the country; may be affected by historical and cultural relationships17. In our country, the wars, medical tourism, and Cross border transfer of patients particularly incoming workers might play a significant role in emerging and dissemination of different variants of carbapenemase encoding genes. There is an urgent need to find guidelines and appropriate procedures of infection control in order to deny such infections among patients.
Acknowledgments
The authors thanks Mustansiriyah University (http://uomustansiriyah.edu.iq/) for its support during the tenure of this work.
Conflict Of Interest
The authors declare that there is no conflict of interest.
Authors’ Contribution
SH designed the experiments and analyzed the data. NH performed the experiments and wrote the manuscript. SH read and approved the manuscript.
Funding
None.
Data Availability
The datasets of 16S rDNA gene, blaVIM-2 gene, blaOXA-48 gene and blaNDM gene sequences from this study were deposited in NCBI database under accession numbers MK182251 to MK182258, MK156197 to MK156202 and MK159338 to MK159352. All relevant data are available from the authors upon request.
Ethics Statement
This article does not contain any studies with human participants or animals performed by any of the authors.
- Patel G., Robert A. Bonomo. Status report on carbapenemases: challenges and prospects. Expert Rev AntiInfect Ther, 2011; 9(5): 555-570.
- Poirel L., Johann D. Pitout, Patrice N. Carbapene-mases: molecular diversity and clinical consequences. Future Microbiol.,2007; 2: 501–512.
- Dos Santos G.S., E.G. Solidonio, M.C.V.V. Costa, ROAMelo, I.F.A.C. Souza, GRSilva, K.X.F.R. Sena. Study of the Enterobacteriaceae group CESP (Citrobacter, Enterobacter, Serratia, Providencia, Morganella and Hafnia): a review,”in The Battle Against Microbial Pathogens: Basic Science, Technological Advances and Educational Programs, ed A. Mיndez-Vilas (Badajoz: Formatex),2015; 2: 794-805.
- Tarashi S., Hossein G., Soroor E., Ali P., Ali H. Phenotypic and molecular detection of Metallo-beta-lactamase genes among imipenem resistant Pseudomonas aeruginosa and Acinetobacter baumannii strains isolated from patients with burn injuries. Arch. Clin. Infect. Dis., 2016; 11(4): 1-6.
- Nordmann P. Carbapenemase-producing Entero-bacteriaceae: overview of a major public health challenge. Mיd. Mal. Infect., 2014; 44: 51–56.
- Bush K., Megan P., John L. Lock, Anne MQueenan, James HJorgensen, Ryan MLee, James SLewis, Deidre J. Detection systems for carbapenemase gene identification should include the SME serine carbapenemase. Intern. J. Antimicrob. Agents, 2013; 41(1): 1-4.
- Thomson K.S. Extended-spectrum-b-lactamase, AmpC, and carbapenemase issues. J. Clin. Microbiol., 2010; 48(4): 1019-1025.
- Iraz M., Azerײ D zg n, Cemal S., Mehmet Z. Doymaz, Yasemin Akkoyunlu, Ayseg l S., Anton Y. Peleg, Osman B. ײzg m s, FatihSBeris, Hakan K., Ayseg lַַiחek. Distribution of b-lactamase genes among carbapenem-resistant Klebsiella-pneumoniae strains isolated from patients in Turkey. Ann. Lab. Med., 2015; 35(6): 595-601.
- Nordmann P., Thierry N., Laurent P. Global spread of carbapenemase-producing Enterobacteri-aceae. Emer Infect Dis., 2011; 17(10): 1791.
- Atlas R. M., Parks L.C., Brown A.E. 1995. Laboratory manual of experimental microbiology. Mosby-Year Book Inc.
- Clinical and laboratory standards institute. 2016. Performance standards for antimicrobial susceptibility testing.26th Edition. Supplement M100S. CLSI, Wayne, PA.
- Poirel L., Timothy R. Walsh, Vincent C., Patrice N. Multiplex PCR for detection of acquired carbapenemase genes. Diag. Microbiol. Infect. Dis., 2011; 70(1): 119-123.
- Spilker T., Tom C., Peter V., John J. LiPuma. PCR-based assay for differentiation of Pseudomonas aeruginosa from other Pseudomonas species recovered from cystic fibrosis patients. J. Clin. microbiol, 2004; 42(5): 2074-2079
- Magray M.S.U.D., Anup K., Anil K. Rawat, Shipra S. Identification of Escherichia coli through analysis of 16S rRNA and 16S-23S rRNA internal transcribed spacer region sequences. Bioinformation, 2011; 6(10): 370-371.
- Bonnin R.A., Thierry N., Laurent P., Patrice N. Phenotypical-, biochemical-and molecular-based techniques for detection of metallo-b-lactamase NDM in Acinetobacter baumannii. J. Clin. Microbio., 2012; 50(4)1419-1421.
- Khalifa H.O., Ahmed M. Soliman, Ashraf M. Ahmed, Toshi S., Toshinori H., MitsuyasuI, YutaK, Shizuo K., Motoyuki S., Tadashi Tadashi S. High carbapenem resistance in clinical gram-negative pathogens isolated in Egypt. Microb. Drug Resist., 2017; 23(7): 838-844.
- Leylabadlo H.E., Mohammad A., Mohammad A. Dissemination of carbapenemases producing Gram negative bacteria in the Middle East. Iran J. Microbiol, 2015; 7(5): 226.
- Adler A., Maya S., Mitchell J. Schwaber, Shiri N.-V., Yacoub D., Rotem E., Ester S., Shmuel B., Samira M., Yehuda C. Introduction of OXA-48-producing Enterobacteriaceae to Israeli hospitals by medical tourism. J. antimicrob. chemother, 2011; 66(12): 2763-2766.
- Abdulla A.A., Hussein O.M. Al-Dahmoshi, Thikra A. Abed. Wurood H. Muttaleb. Characterization of Multidrug Resistant Carbapenemases-Producing Escherichia coli and Klebsiella pneumoniae Isolates from Urinary Tract Infection. J. Chem. Pharm. Scie, 2016; 9(3): 1116-1120.
- Zowawi H.M., Anna L. Sartor, Hanan H. Balkhy, Timothy R. Walsh, Sameera M.A.l. Johani, Reem Y. AlJindan. Molecular characterization of carbapenemase-producing Escherichia coli and Klebsiella pneumoniae in the countries of the Gulf cooperation council: dominance of OXA-48 and NDM producers. Antimicrob Agents Chemother, 2014; 58: 3085-90.
- Moubareck C.A., Shaimaa F. Mouftah, Tibor P., Akela G., Dalal H. Halat, Anju N., Mouza A. AlSharhan, etal. Clonal emergence of Klebsiella pneumoniae ST14 co-producing OXA-48-type and NDM carbapenemases with high rate of colistin resistance in Dubai, United Arab Emirates. Intern. J. Anti. microb. Agents, 2018; 52(1): 1-6.
- Dandachi I, SalemESokhn,ElieN, EidA.ZiadD. Carriage of beta-lactamase-producing Enterobacteriaceae among nursing home residents in north Lebanon. Intern. J. Infect. Dis, 2016; 45: 24-31.
- Mohamed S.R., Alfadil A., Wafa MHussien, Mohamed I. Saeed. blaOXA-48Carbapenem Resistant Pseudomonas aeruginosa Clinical Isolates in Sudan. J. Adv. Microbiol., 2018; 10(4): 1-5.
- Dortet L., Gaelle C., Patrice N. Dissemination of carbapenemase-producing Enterobacteriaceae in France, 2012. J. Anti. microb. Chemother, 2013; 69(3): 623-627.
- Dortet L., Mirela Fl, Yves-Marie Bl, Elodie Cl, Sandrine Bl, Anaןs Vl, Thierry N. Dissemination of carbapenemase-producing Enterobacteriaceae and Pseudomonas aeruginosa in Romania. Anti. microb. Agents Chemother., 2015; 59(11): 7100-7103.
- Mataseje L.F., David A. Boyd, Jeffrey F., David H., Linda H., et al. Characterization of OXA-48-like carbapenemase producers in Canada, 2011–14. J. Antimicrob. Chemother, 2017; 73(3):626-633.
- AL_Jubori S.S., Israa M. AL_Kadmy, Zuhar J. Al_Ani. Emergence of multidrug resistance (MDR) Acinetobacter baumannii isolated from Iraqi hospitals. Adv. Environ. Biol., 2016; 10(5):265-276.
- Hammadi A.H., Najlaa N. Yaseen, Harith JF Al-Mathkhury. Molecular Detection of Some b-lactamases Genes in Uropathogenic Escherichia coli. Iraqi J.Sci., 2015; 56(3A): 1925-1931.
- Djahmi N., Catherine D.-R.,AlixP, Mazouz D., Albert S., Jean-Philippe L. Epidemiology of carbapenemase-producing Enterobacteriaceae and Acinetobacter baumannii in Mediterranean countries. Bio. Med. res. int., 2014. http://dx.doi.org/10.1155/2014/305784.
- Guerin F., Corneliu H., Gabriella S., Odile L., Dominique S.-C., Claire. Bacterial prostatitis due to Pseudomonas aeruginosa harbouring the blaVIM-2 metallo-b-lactamase gene from Saudi Arabia. J. Antimicrob. Chemother, 2005; 56(3): 601-602.
- Rajabnia R., Fariba A., Elaheh Ferdosi Shahandashti, Zahra M. Nosocomial emerging of (VIM1) carbapenemase-producing isolates of Klebsiella pneumoniae in North of Iran. Iran J. Microbiol., 2015; 7(2): 88-93.
- Haciseyitoglu D., Aysegul D., Ayham A., Fatma E., Yasemin C., Serdar O., Zerrin A. The First Entero-bactercloacae Co-Producing NDM and OXA-48 Carbapenemases and Interhospital Spread of OXA-48 and NDM-Producing Klebsiell-apneumoniae in Turkey. Clin. Lab. , 2017; 63(7): 1213-1222.
- Hammami S., Boutiba-Ben B.R.Ghozzi, M. Saidani, S. Amine, S. Ben Redjeb. Nosocomial outbreak of imipenem-resistant Pseudomonasaeruginosa producing VIM-2 metallo-b-lactamase in a kidney transplantation unit. Diag. pathol, 2011; 6(1): 106.
- Mereuד AI, Aida CBדdescu, Olivia S. Dorneanu, Luminia SIancu, Cristina GTuchilus. Spread of VIM-2 metallo-beta-lactamase in Pseudomonas aeruginosa and Acinetobacter baumannii clinical isolates from Iasi, Romania. Rom Rev. Lab. Med., 2013; 21(4): 423-430.
- Hong JS, Eun-Jeong Y, WonkeunS, Yu BSeo,SaeamS, Min-Jeong P, Seok HJeong, KyungwonL. Molecular Characterization of Pseudomonas putida Group Isolates Carrying blaVIM-2 Disseminated in a University Hospital in Korea. Microbial Drug Resist,2018; 24(5): 627-634.
- Touati M., Seydina M. Diene, Mazouz D., Abdelghani D., Abdelkarim R., Jean-Marc R. Dissemination of class I integron carrying VIM-2 carbapenemase gene in Pseudomonasaeruginosa clinical isolates from intensive care unit of university hospital of Annaba, Algeria. Antimicrob. Agents and Chemother., 2013; 57(5): 2426-2427.
- Kazi M., Drego L., Chaitali N., Kanchan A., Rajeev S., Anjali S., C. Rodrigues. Molecular characterization of carbapenem-resistant Enterobacteriaceae at a tertiary care laboratory in Mumbai. Eur. J. Clin. Microbiol. Infect. Dis., 2015; 34(3): 467-472.
- Alshara J.M.R., Zuhair S.R. Alsehlawi, Dheyaa S.A. Aljameel, Zeena S. Al-Zubbedy, Ali MAlmohana. First report of New Delhi metallo-beta-lactamase (NDM-1) producing Pseudomonas aeruginosa in Iraq. J. Biol. Agricul. Healthcare, 2014; 4: 40-7.
- Al-Harmoosh R.A., Eman M. Jarallah. First Detection of the blaNDM-1 and blaNDM-2 Genes IN a Clinical Isolates of Acinetobacter baumannii in Hillah Hospitals-Iraq. Int. J. Adv. Res., 2015; 3(10): 1407-1416.
- Hussein N.H. Genotypic Detection of Carbapenem- Resistant Escherichia coli Producing NDM-1 Gene for the First Time in Baghdad/Iraq. J. Glob. Pharma. Tech., 2017; 09(9): 106-111.
- Hammoudi A.A., Azhar N. Hussein, Mohammed S. Jebur. Detection of blaNDM -Metallo-b-Lactamase Genes in Klebsiella pneumoniae Strains Isolated From Burn Patients in Baghdad Hospitals. Med.J. Babylon, 2016; 13( 4): 904 – 913.
- Nordmann P., Laurent D., Laurent P. Carbapenem resistance in Enterobacteriaceae: here is the storm!. Trends Mol. Med.,2012; 18(5): 263-272.
- Sonnevend ֱ., Akela A. Ghazawi, Rayhan H., Wafaa J., Vincent O. Rotimi, Atef M. Shibl, Amina A., et al. Characterization of carbapenem-resistant Enterobacteriaceae with high rate of auto-chthonous transmission in the Arabian Peninsula. PLoS One, 2015; 10(6): e0131372.
- Ben Helal R., Raoudha D., Meriem C., Naouel K., Farouk B., Mohamed S. El Asli, Mohamed B. Moussa. Occurrence and Characterization of Carbapenemase-Producing Enterobacteriaceae in a Tunisian Hospital. Microb. Drug Resist., 2018; 24(9): https://doi.org/10.1089/mdr.2018.0013
- Khatun R., Shamsuzzaman S.M. Detection of OXA-181/OXA-48 carbapenemase producing Entero-bacteriaceae in Bangladesh. Ibrahim Med. Coll. J., 2015; 9(2): 45-51.
- Ageevets VA, Irina VPartina, Eugenia SLisitsyna, Elena NIlina, Yuri VLobzin, Sergei A. Shlyapnikov, Sergei VSidorenko. Emergence of carbapenemase -producing Gram-negative bacteria in Saint Petersburg, Russia. Int. J. Antimicrob. Agents., 2014; 44(2): 152-155.
- Meletis G.,Dimitrios C., Nikos M. Double-and multi-carbapenemase-producers: the excessively armored bacilli of the current decade. Eur. J. Clin. Microbiol. Infect. Dis., 2015; 34(8): 1487-1493
- Jamal W.Y., M.J. Albert, Vincent O. Rotimi. High prevalence of new delhimetallo-b-lactamase-1 (NDM-1) producers among carbapenem-resistant Enterobacteriaceae in Kuwait. PloS one, 2016; 11(3), https://doi.org/10.1371/journal. pone.0152638.
- Doi Y., Jessica A. O’Hara, James F. Lando, Ashley M. Querry, Bethany M. Townsend, Anthony W. Pasculle, Carlene A. Muto. Co-Production of NDM-1 and OXA-232 by Klebsiella pneumoniae. Emerg. Infect. Dis., 2014; 20(1): 164-165.
- Bousquet, Aurore, Marion Duprilot, Didier Moissenet, BיatriceSalauze, JיrפmeRambaud, etal. “First case of multidrug-resistant blaNDM-1-and blaOXA-232-carrying Klebsiella pneumoniae and its probable cross-transmission in a French hospital.” Int. J. Antimicrob. Agents, 2014; 44( 5): 469-470.
- Lin K.Y., Tsai-Ling L., Jann-Tay W., Shan-Chwen C.Carbapenem-resistant Pseudomonas aeruginosa in Taiwan: Prevalence, risk factors, and impact on outcome of infections. J. Microbiol. Immun. Infect., 2016; 49(1):52-59.
© The Author(s) 2019. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.