


ISSN: 0973-7510
E-ISSN: 2581-690X
Mohammed Fauzi Abdul Rani2, Mariam Mohamad3
Ariza Adnan4
The dynamics and protectiveness of the hybrid immune responses, especially in individuals who have experienced severe COVID-19, remain to be fully understood. This study aims to identify the prevalence and persistence of neutralising antibodies throughout time, and to investigate the longitudinal profile of anti-SARS-CoV-2 IgG antibodies targeting the receptor binding domain (RBD) in patients recovering from severe COVID-19. A total of 42 hospitalised COVID-19 survivors were enrolled from three medical centres in Malaysia. Serial blood samples were collected at four time points post-discharge (approximately 90, 180, 270 and 360 days). IgG titres were quantified using ELISA and neutralising antibodies (NAbs). Statistical analyses were performed to explore antibody dynamics and correlations. Among 42 participants, 24 completed all four visits. Mean antibody titre showed an initial decline after the first visit, followed by a gradual increase over time, with the highest being at Visit 4 (360-390 days post-discharge). The highest titre (266.7 ± 30.9 BAU/mL) was observed in a recipient, 10 days after receiving the fourth vaccination. All participants except one demonstrated protective NAbs at the final visit. Higher BMI was significantly associated with disease severity (P = 0.006), while IgG titres were higher in individuals with more severe initial infections (Category 5). This study highlights the persistence of antibody response with hybrid immunity, with the booster vaccinations contributing to increased antibody titres. RBD-specific IgG titres provide useful insights into their trends, while the concurrent NAbs assessment is important for a comprehensive understanding of the protective efficacy following hybrid immunity.
COVID-19, Neutralising Antibodies, Immunoglobulin G (IgG), Hybrid Immunity, Antibody Persistence, Booster Vaccination, ELISA
The coronavirus disease 2019 (COVID-19) was declared a global pandemic by the World Health Organization (WHO) due to its significant impact on public health, resulting in high morbidity and mortality worldwide.1,2 As of December 7, 2025, over 778 million confirmed cases and more than 7 million deaths had been reported globally.3 The virus spreads efficiently due to its wide spectrum of clinical manifestations, ranging from asymptomatic to severe pneumonia and multiorgan failure.
To classify disease severity, WHO guidelines have been widely adopted. Patients with mild illness (Categories 1-3) typically experience asymptomatic or upper respiratory symptoms, whereas those in Categories 4 and 5 require oxygen therapy or intensive care, including cases of respiratory failure, septic shock, or multiorgan dysfunction.4 High-risk individuals, including the elderly and those with comorbidities such as cardiovascular disease, diabetes, cancer, and immunosuppression, are more likely to develop severe disease.5
To curb transmission and reduce disease burden, initial control strategies included movement control orders (MCOs), mask-wearing, social distancing, and enhanced hygiene protocols. The introduction of COVID-19 vaccines in February 2021 under Malaysia’s National Immunisation Program marked a pivotal advancement in preventive efforts.6
From an immunological perspective, SARS-CoV-2 infection elicits a humoral immune response marked by the production of virus-specific antibodies. These antibodies typically target the spike (S) protein, especially the receptor-binding domain (RBD), which is crucial for viral entry into host cells.7,8 Of the three major immunoglobulin classes, IgA, IgM, and IgG, IgG is the most stable and long-lasting. Its kinetics typically show a peak between 16 and 30 days post-infection and persist for months to years.9-12
Notably, higher antibody titres have been reported in individuals who experienced severe disease compared to those with mild or asymptomatic.12-14 However, with the advent of COVID-19 vaccines and the widespread occurrence of hybrid immunity (from both infection and vaccination), antibody dynamics have become more complex. In addition to binding antibodies like IgG, neutralising antibodies (NAbs) play a vital role in protective immunity by preventing viral entry into host cells.15 The surrogate virus neutralisation test (sVNT) offers a practical way to assess this function without the need for live virus.16
Reinfections and breakthrough infections continue to occur, often driven by emerging SARS-CoV-2 variants capable of immune evasion.17-19 Therefore, understanding the durability and quality of post-infection and post-vaccination antibody responses is critical. This study aims to investigate the longitudinal dynamics of anti-SARS-CoV-2 (RBD) IgG antibody levels in convalescent individuals who had recovered from severe COVID-19, and to explore associations between antibody responses and demographic or clinical characteristics, including vaccination status. The findings will contribute to our understanding of long-term protective immunity and may inform vaccine booster strategies for high-risk populations.
Study design, setting and participants
Study designs
This observational study aimed to evaluate the longitudinal dynamics of IgG antibodies targeting the SARS-CoV-2 receptor-binding domain (RBD) in convalescent COVID-19 patients. Specifically, it involved serial measurement of antibody titres at multiple time points to assess their levels, temporal changes, and neutralising activity. The study also sought to explore potential associations with sociodemographic and clinical factors, including vaccination status.
Participants and setting
Eligible participants were adult (≥18 years) COVID-19 survivors who had experienced severe disease (Category 4 or 5) and had been hospitalised in 2021 at one of the following centres: Hospital Sungai Buloh (HSB), Hospital Al-Sultan Abdullah (HASA) or UiTM Private Specialist Centre (UPSC). COVID-19 diagnosis was confirmed via real-time reverse transcriptase polymerase chain reaction (RT-PCR). The study was conducted between 6 October 2021 and 3 August 2022, during which the predominant circulating SARS-CoV-2 variant was Delta (October to December 2021), followed by Omicron, which became dominant from approximately February to August 2022.
Participants with post-COVID-19 infections were recruited during their follow-up appointments for pulmonary function assessment at the HASA Respiratory Clinic, within three months after hospital discharge. Each participant was followed for a period of one year. A 5 mL venous blood sample was collected at four pre-defined time points, i.e. Visit 1 (baseline) at the time of recruitment, which was 90-120 days, followed by Visit 2 (180-210 days), Visit 3 (270-300 days), and Visit 4 (360-390 days) post-admission, respectively. Blood samples were obtained either during clinic appointments or via home visits, depending on participant convenience. All participants received one to four doses of COVID-19 vaccine in addition to natural immunity from prior infection. The first two doses constituted the primary vaccination series, while the third and fourth doses were considered boosters. All participants received homologous vaccines, i.e. CoronaVac for both primary and booster doses, except for one participant who received a heterologous regimen, i.e. CoronaVac for the primary series followed by BNT162b2 as the booster.
Sample size calculation
During the study period, approximately 500 post-severe COVID-19 patients were followed up at the HUiTM Respiratory Clinic. The sample size was calculated using the single proportion formula via the OpenEpi sample size calculator. Based on a study conducted in China reporting an overall positivity rate of 98.7% among severe cases, and assuming a 95% confidence level with a 5% margin of error, the minimum required sample size was estimated to be 20 participants.
Data collection
A structured questionnaire was used to collect the following demographic and clinical data: Age, gender, and body mass index (BMI), Presence of chronic conditions (e.g., hypertension, diabetes mellitus, Smoking status, and COVID-19 vaccination status. The reinfection status was also included based on patients’ commercial RTK results (rapid test kit).
Inclusion criteria
Participants (>18 years old) who consented to be enrolled in the study.
Exclusion criteria
Participants were excluded if they had COVID-19 severity Category 3 or below, more than 3 months post COVID-19 infection discharge, did not provide informed consent or defaulted on follow-up or could not be contacted for subsequent visits.
Quantitative assay of Anti-SARS-CoV-2 IgG against RBD protein antibody titre using (ELISA) and Neutralising antibody (Nabs) using sVNT
We performed the detection of anti-SARS-CoV-2 IgG antibodies using a quantitative enzyme-linked immunosorbent assay (ELISA) (Wantai BioPharm, China) according to the manufacturer’s instructions. It measures IgG antibodies targeting the receptor-binding domain (RBD) of SARS-CoV-2. The results were expressed as mean antibody titre and reported in Binding Antibody Units per millilitre (BAU/mL).
In addition, neutralising antibody (NAbs) activity was assessed using the SARS-CoV-2 Surrogate Virus Neutralisation Test (sVNT) Kit (GenScript, USA), following the manufacturer’s protocol. A cut-off value of >30% inhibition was used to define a positive (protective) result, with values ≤30% considered negative. These laboratory tests were performed after each visit.
Statistical analysis
Statistical analysis was assumed significant if P-values were below 0.05. All analyses were conducted using SPSS Statistics software version 29 (IBM SPSS Inc.) and GraphPad Prism (version 8.4.2, GraphPad Software, San Diego, CA, USA) was used to draw the graphs and scatter plots. The participants’ clinical characteristics were summarised using descriptive analysis. Categorical variables were reported as frequencies and percentages.
Ethics approval and consent to participate
The study was conducted in compliance with the tenets of the Helsinki Declaration and approved by the Research Ethics Committee (REC) of Universiti Teknologi MARA (Reference No. REC/08/2021 FB/49). Written informed consent was obtained from all participants prior to their involvement.
A total of 62 participants were approached and initially screened for recruitment. However, 20 individuals were excluded on the day of recruitment for the following reasons: one participant had a Category 3 COVID-19 infection, four participants had been discharged for more than 4 months, and 15 declined to provide informed consent. This resulted in 42 participants being officially enrolled in the study, all of whom provided baseline blood samples.
During follow-up, nine participants withdrew before the first follow-up (Visit 2), primarily due to work commitments, reducing the cohort to 33 participants. Four more participants withdrew before the third visit, leaving 29 participants. Five additional participants withdrew before the final visit, resulting in 24 participants who completed the full 12-month blood sampling schedule. In total, 18 participants withdrew over the course of the study, nine before the second collection, 4 before the third, and 5 before the final (Figure 1).
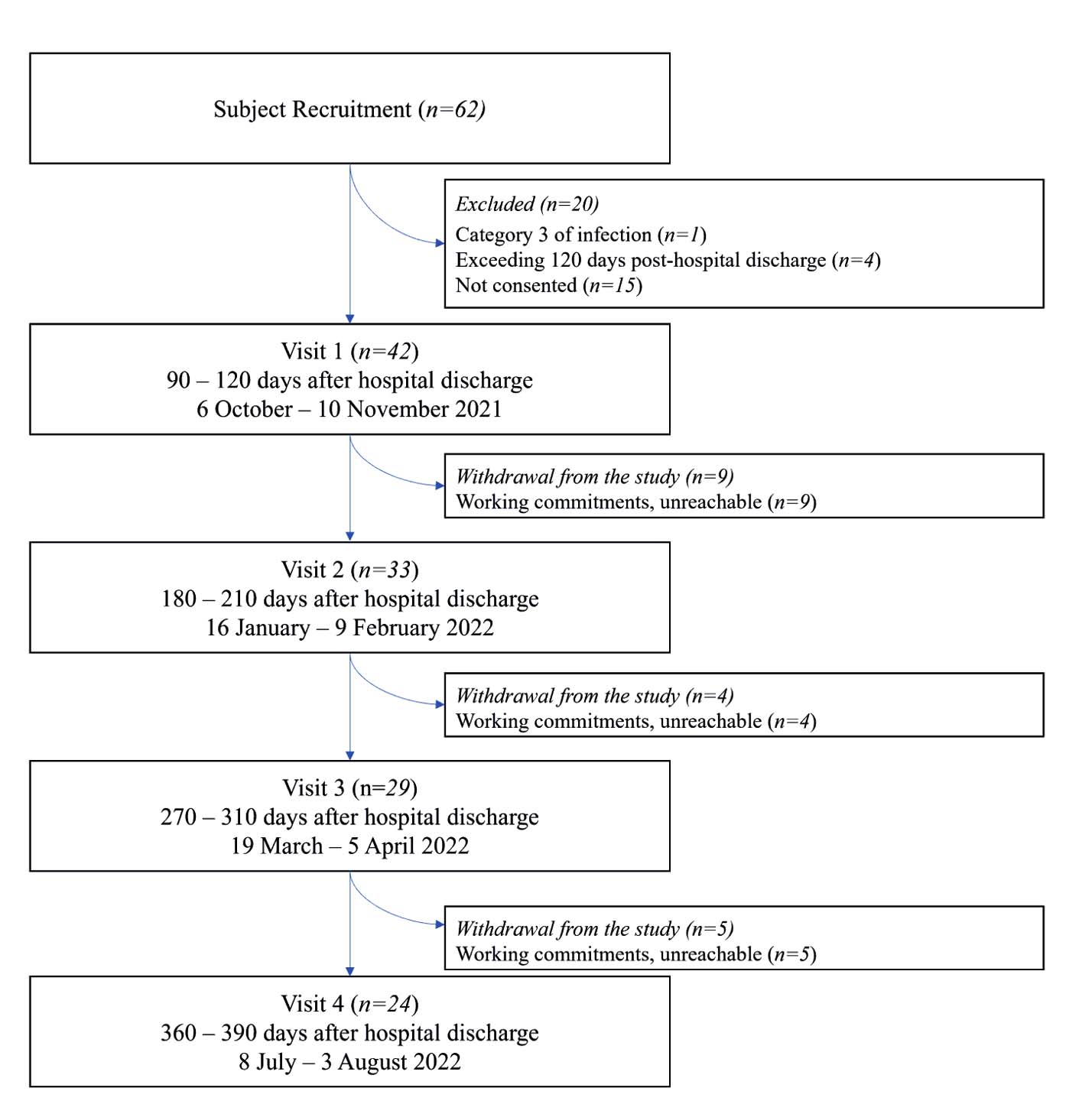
Figure 1. Summary of the subjects’ enrolment for the study
Demographic and clinical characteristics were analysed. Out of 42 participants, there were 22 (52.4%) with Category 4 COVID-19 and 20 (47.6%) with Category 5 COVID-19. Among those in Category 4, 15 (57.7%) were male, and 7 (42.3%) were female. Among Category 5 participants, 11 (55.0%) were male and 9 (45.0%) were female. For age, the mean age in Category 4 was 48.1 years, with 36.4% aged 40 years or below. In Category 5, the mean age was 49.7 years, with only 15% aged 40 years or below. The mean BMI was 30.4 in Category 4 and 33.4 in Category 5. In Category 4, 31.8% were underweight or normal, and 68.2% were overweight or obese. There is a significant difference in BMI category between Category 4 and Category 5 of COVID-19 infection (p = 0.006), where all participants in Category 5 were overweight or obese (100%). Hypertension was reported in four participants from each group (18.2% in Category 4, 20.0% in Category 5). Diabetes mellitus was reported in three participants in Category 4 (13.6%) and 4 in Category 5 (20.0%). In Category 4, 11 participants (50%) had received 1 or 2 doses, and 11 (50%) had received 3 or 4 doses. In Category 5, 13 participants (65%) had received one or two doses, and seven (35%) had received three or four doses. For smoking status, none of the Category 4 participants were smokers, while one participant (5%) in Category 5 was a smoker. Four participants had reinfection throughout the study follow-up, but these differences were not significant (Table 1).
Table (1):
Baseline demographic and clinical data of participants in this study
| Total n = 42 | Category | P-value | ||||
|---|---|---|---|---|---|---|
| 4 (n = 22) | % | 5 (n = 20) | % | |||
| Age (years) | ||||||
| Mean ± SD | 49 ± 12.03 | 48.1 ± 14.6 | – | 49.7 ± 8.3 | – | 0.166b |
| <40 | 11 | 8 | 36.4 | 3 | 15.0 | |
| >40 | 31 | 14 | 63.6 | 17 | 85.0 | |
| Gender | ||||||
| Male | 26 | 15 | 57.7 | 11 | 42.3 | 0.527b |
| Female | 16 | 7 | 41.2 | 9 | 52.9 | |
| BMI | ||||||
| Mean ± SD | 31.9 ± 1.5 | 30.4 ± 6.7 | – | 33.4 ± 4.7 | – | 0.006a |
| Underweight & Normal | 7 | 7 | 31.8 | 0 | 0 | |
| Overweight & Obese | 35 | 15 | 68.2 | 20 | 100 | |
| Chronic illness | ||||||
| Hypertension | 8 | 4 | 18.2 | 4 | 20.0 | 1.000b
1.000b |
| Diabetes mellitus | 7 | 3 | 13.6 | 4 | 20.0 | |
| Smoking status | ||||||
| Yes | 1 | 0 | 0 | 1 | 5.0 | 0.476b |
| No | 41 | 22 | 100 | 19 | 95.0 | |
| Vaccination status | ||||||
| 1 | 1 | 1 | 4.5 | – | – | Not tested |
| 2 | 23 | 10 | 45.5 | 13 | 65.0 | |
| 3 | 15 | 10 | 45.5 | 5 | 25.0 | |
| 4 | 3 | 1 | 4.5 | 2 | 10.0 | |
| Reinfection | ||||||
| Yes | 4 | 4 | 18.2 | 0 | 0 | 0.233b |
| No | – | 18 | 81.8 | 20 | 100 | |
BMI: body mass index (<18.5: underweight, 18.5-24.9: normal, 25.0-29.9: overweight, ≥30.0: obese).
a: Pearson’s Chi-Square; b: Fisher’s Exact Test
Of 42 participants, 24 (57.1%) were completers and 18 (42.9%) were non-completers (participants who defaulted from the study at any visit). Among the completers, 14 (58.3%) were male, and 10 (41.7%) were female, as compared to 12 (22.2%) male and six (33.3%) female among non-completers. The mean age ± SD of the completers was 46.54 ± 11.24 years, with 70.8% aged >40 years, while the non-completers had a mean age of 51.94 ± 12.40 years, with 77.8% aged >40 years. The mean BMI ± SD was 32.72 ± 5.49 among completers and 30.21 ± 6.27 among non-completers. Among completers, three (12.5%) participants were underweight or normal weight, while 21 (87.5%) were overweight or obese. Similarly, among non-completers, only three (16.7%) were underweight or normal weight and 15 (83.3%) were overweight or obese. Unlike the comparison across COVID-19 infection categories (Table 1), the BMI distribution between completers and non-completers was not statistically significant (P = 1.000). Among completers, eight (33.3%) reported hypertension and 6 (25.0%) reported diabetes mellitus, whereas among non-completers, five (27.7%) and 4 (22.2%) reported hypertension and diabetes mellitus, respectively. Only 1 completer (4.2%) reported being a smoker, while none of the non-completers were smokers. Regarding vaccination status, among completers 8 (33.3%), 13 (54.2%), and 3 (12.5%) participants had received two, three, and four doses, respectively. In contrast, among non-completers, the majority (15 participants, 83.3%) had received two doses, followed by 2 (11.1%) who had received three doses, and 1 (5.6%) who had received one dose; no four-dose recipients were observed. All four reinfection cases (16.7%) reported in this study occurred among completers (Table 2).
Table (2):
Baseline demographics between completers and non-completers in this study
| Completers | Non-completers | P-value | |||
|---|---|---|---|---|---|
| (n = 24) | % | (n = 18) | % | ||
| Age (years) | |||||
| Mean ± SD | 46.54 ± 11.24 | – | 51.94 ± 12.40 | – | 0.731b |
| <40 | 7 | 29.2 | 4 | 22.2 | |
| >40 | 17 | 70.8 | 14 | 77.8 | |
| Gender | |||||
| Male | 14 | 58.3 | 12 | 66.7 | 0.819a |
| Female | 10 | 41.7 | 6 | 33.3 | |
| BMI | |||||
| Mean ± SD | 32.72 ± 5.486 | 12.5 | 30.21 ± 6.268 | – | 1.000b |
| Underweight & Normal | 3 | 3 | 16.7 | ||
| Overweight & Obese | 21 | 87.5 | 15 | 83.3 | |
| Chronic illness | |||||
| Hypertension | 8 | 33.3 | 5 | 27.7 | 0.962a |
| Diabetes mellitus | 6 | 25.0 | 4 | 22.2 | 1.000b |
| Smoking status | |||||
| Yes | 1 | 4.2 | 0 | – | 1.000b |
| No | 23 | 96.8 | 18 | 100 | |
| Vaccination status | |||||
| 1 dose | – | – | 1 | 5.6 | Not tested |
| 2 doses | 8 | 33.3 | 15 | 83.3 | |
| 3 doses | 13 | 54.2 | 2 | 11.1 | |
| 4 doses | 3 | 12.5 | – | – | |
| Reinfection | |||||
| Yes | 4 | 16.7 | 0 | – | 0.122b |
| No | 20 | 83.3 | 18 | 100 | |
BMI: body mass index (<18.5: underweight, 18.5-24.9: normal, 25.0-29.9: overweight, >30.0: obese).
a: Pearson’s Chi-Square; b: Fisher’s Exact Test
During Visit 1, four participants (4/42) (9.5%) had received only one dose, and 38 participants (90.5%) had received two doses. During Visit 2, one participant (1/33) (3.0%) had one dose, 23 participants (23/33) (69.7%) had two doses, and nine participants (9/33) (27.3%) had three doses. During Visit 3, one participant (1/29) (3.4%) had one dose, 11 participants (11/29) (37.9%) had two doses, and 17 (17/29) participants (58.6%) had three doses. During the final visit, three participants (3/24) (12.5%) had four doses, 13 (13/24) participants (54.2%) had three doses, and 8 participants (8/24) (33.3%) had two doses. The mean timing between vaccination and the blood collection during Visit 1 was shorter for the one-dose recipients at 29.5 ± 23.81 days as compared to two-dose recipients (44.76 ± 20.97). During Visit 2, three-dose recipients had a lower mean time interval at 25.33 ± 16.02 days, in comparison to those receiving two doses of vaccination at 124.70 ± 22.68 days. We observed the same trend during Visit 3, where the participants who received three doses of vaccines had a lower mean time between immunisation and visit (69.29 ± 32.02 days versus 191.0 ± 15.56 days). Lastly, at Visit 4, the lowest mean time between vaccination and visit was reported for the four-dose recipients, at 20.67 ± 22.03 days. These changes reflect the progression of booster dose uptake over the course of the study (Table 3).
Table (3):
Vaccine doses per participant in each visit
| Visit 1 | Visit 2 | Visit 3 | Visit 4 | ||
|---|---|---|---|---|---|
| (90-120 days) | (180-210 days) | (270-310 days) | (360-390 days) | ||
| Participant | n | 42 | 33 | 29 | 24 |
| Doses of vaccinations | n (%) | ||||
| 1 | – | 4 (9.5%) | 1 (3.0%) | 1 (3.4%) | N/A |
| 2 | – | 38 (90.5%) | 23 (69.7%) | 11 (37.9%) | 8 (33.3%) |
| 3 | – | N/A | 9 (27.3%) | 17 (58.6%) | 13 (54.2%) |
| 4 | – | N/A | N/A | N/A | 3 (12.5%) |
| Mean days between the most recent vaccination and the blood sampling (Mean ± SD) | – | – | – | – | – |
| 1 | – | 29.50 ± 23.81 | 138 | 209 | N/A |
| 2 | – | 44.76 ± 20.97 | 124.70 ± 22.68 | 191.0 ± 15.56 | 298.80 ± 14.68 |
| 3 | – | N/A | 25.33 ± 16.02 | 69.29 ± 32.02 | 175.00 ± 37.19 |
| 4 | – | N/A | N/A | N/A | 20.67 ± 22.03 |
| COVID-19 Reinfection | n (%) | N/A | 2 (6.1%) | 3 (10.7%) | 4 (16.7%) |
N/A: Not available
Quantitative assay of Anti-SARS-CoV-2 IgG against spike protein antibody titre
The overall mean antibody titre showed a fluctuating pattern, decreasing from Visit 1 to Visit 2, then steadily increasing through Visit 3 and peaking at Visit 4. The highest mean antibody titre (192.5 ± 56.05 BAU/mL) was recorded at Visit 4, where three participants had received their fourth dose an average of 21 days prior. Among two-dose recipients, titres decreased at Visit 2 but rose again in subsequent visits. The highest mean antibody titre in this group was at Visit 1 (172.1 ± 20.5 BAU/mL), while the lowest was at Visit 2 (152.9 ± 17.01 BAU/mL). Three-dose recipients showed a continuous rise in antibody levels from Visit 2 to Visit 4, peaking at 190.2 ± 45.78 BAU/mL in the final visit. Notably, four-dose recipients, though comprising only three individuals at Visit 4, exhibited the highest antibody titres (266.7 ± 30.9 BAU/mL) of all groups and time points (Figure 2).
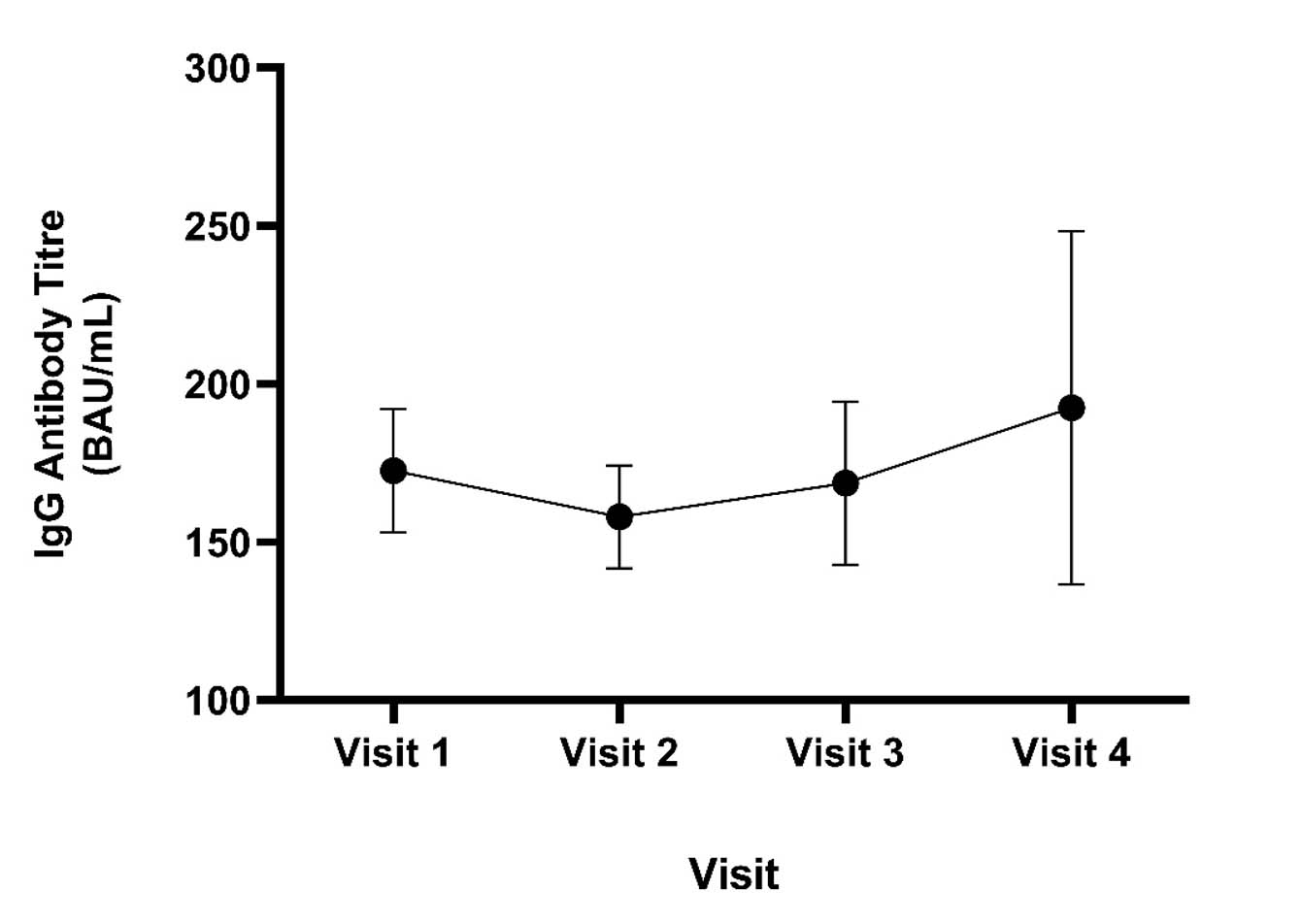
Figure 2. The IgG mean ± SD antibody titre against COVID-19 for all subjects at respective visits representing different time points in Visit 1 to Visit 4
The results revealed a decreasing trend in IgG mean antibody titre in a one-dose recipient from Visit 1 to Visit 3, with the lowest titre recorded at Visit 3 (158.8 BAU/mL). For two-dose recipients, the mean antibody titre declined at Visit 2 compared to Visit 1 but subsequently increased through to Visit 4. The highest mean antibody titre for the two-dose group was observed at Visit 1 (172.1 ± 20.5 BAU/mL), while the lowest occurred at Visit 2 (152.9 ± 17.01 BAU/mL). Among three-dose recipients, a progressively increasing IgG mean antibody titre was recorded from Visit 2 to Visit 4, peaking at 190.2 ± 45.78 BAU/mL during the final visit. The four-dose group, which included only three subjects measured at Visit 4, showed the highest overall IgG titre (266.7 ± 30.9 BAU/mL) compared to all other dose groups and time points (Figure 3).
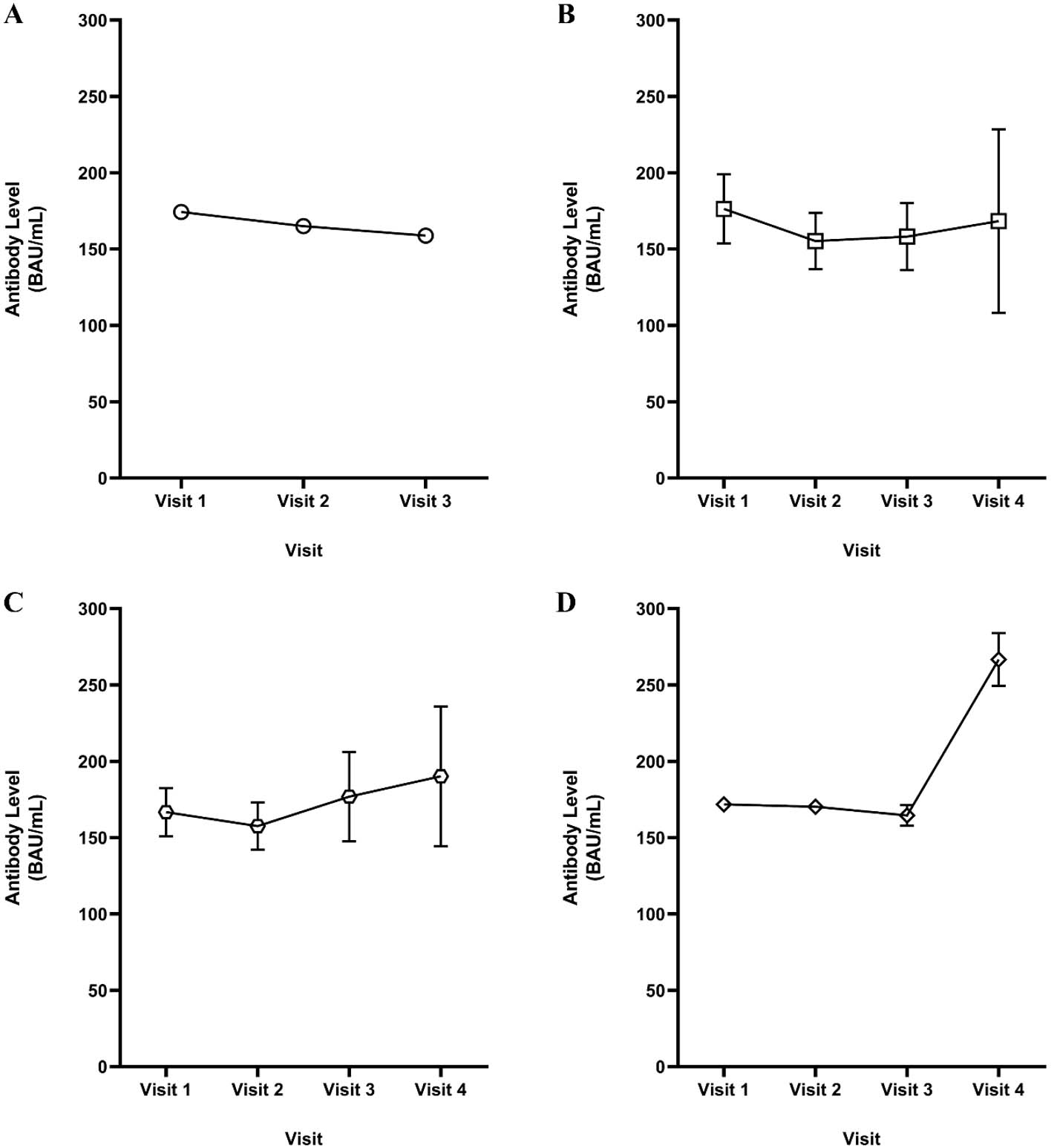
Figure 3. The anti-SARS-CoV-2 spike IgG mean ± SD antibody titre against COVID-19 for recipients of one (A), two (B), three (C) and four (D) vaccination doses at different time points following the hospital discharge
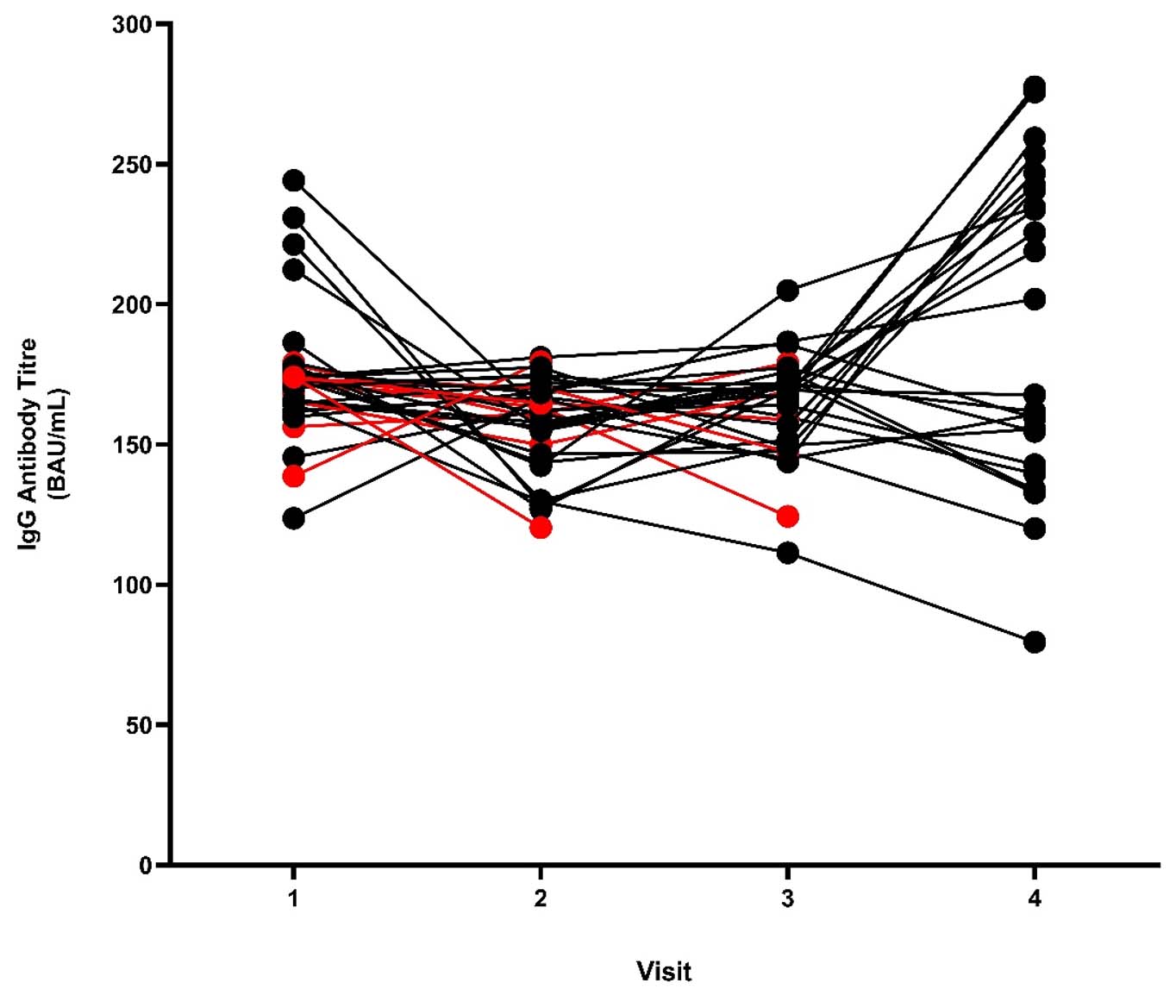
Figure 4. The individual IgG antibody titre against COVID-19 for all subjects at respective visits representing different time points in Visit 1 to Visit 4 (RED: non-completers; BLACK: completers)
Figure 4 shows the individual trajectories of IgG antibody titres across the four visits. Among participants who completed all visits, indicated by the black coloured trajectories, the antibody levels generally fluctuated between Visit 1 and Visit 3, with several individuals showing an increase by Visit 4. Although some participants maintained relatively stable titres over time, noticeable inter-individual variability was observed. Participants who did not complete all visits (red trajectories) exhibited similar fluctuations during the earlier visits. However, their antibody trajectories could only be followed up to the point of dropout, limiting comparison with completers at later time points. Overall, the figure highlights variability in IgG antibody responses over time among the study participants (Figure 4).
We conducted the neutralising antibody (NAbs) testing on all 24 subjects during Visit 4. The results showed protective inhibition rates in all subjects except Subject 3 (two-dose recipient). A cut-off value of >30% inhibition was used to define a positive (protective) result, with values ≤30% considered negative (Figure 5). Subject 3 recorded a negative inhibition rate and also showed a progressive decline in anti-SARS-CoV-2 RBD IgG titres across all four visits, with the lowest level recorded at Visit 4 (79.60 BAU/mL). Among those with protective responses, inhibition rates ranged from 93.57%-95.68%, with a mean of 95.02 ± 0.859.
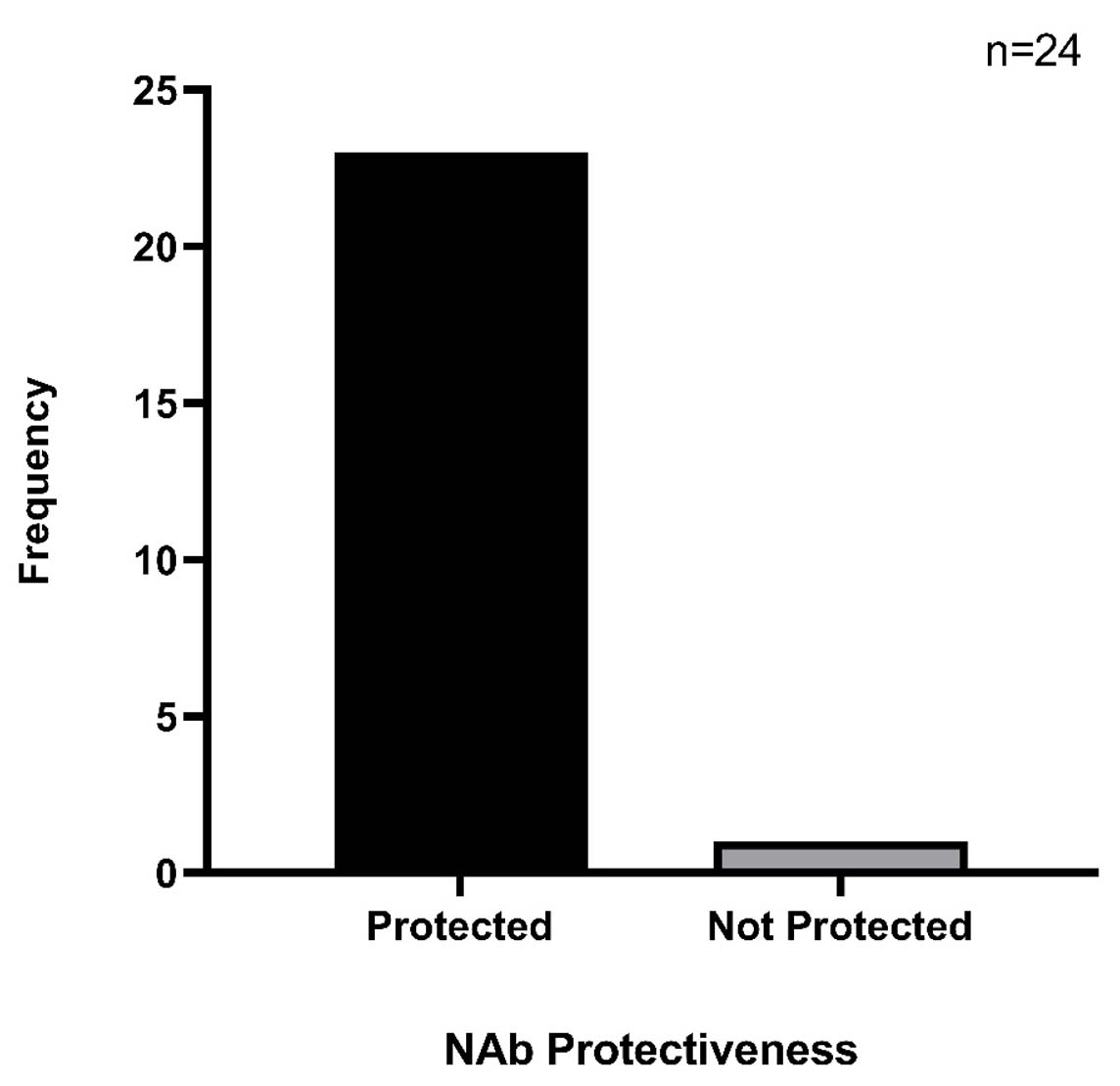
Figure 5. The NAbs presence determination using the sVNT kit
This study involved the follow-up of 42 previously hospitalised COVID-19 patients who had received varying doses of vaccination at different intervals following recovery. However, by the end of the one-year follow-up period, only 24 participants completed all scheduled visits due to exclusion and attrition factors. Attrition is a common challenge in longitudinal studies, particularly those requiring repeated blood sampling or extended commitments from participants. Loss to follow-up can introduce selection bias and reduce statistical power, potentially leading to underestimation of prevalence or weakening of observed associations.20 Nevertheless, our findings showed an increasing trend in antibody titre post-vaccination, which is consistent with the one reported by Haq et al.21 Importantly, well-conducted longitudinal studies with smaller sample sizes can still yield valid and meaningful insights, particularly when data collection is rigorous and participants are well-characterised.22 Despite the reduced cohort size, our data started to show an increase in antibody trends, reflecting the long-term dynamics of IgG and neutralising antibody responses after vaccination and natural infection.
Although our finding for male gender was not significant, the higher proportion of male participants aligns with earlier reports suggesting that men are more likely to experience severe or critical COVID-19 outcomes.23,24 This trend may be attributed to a combination of biological, psychosocial, and behavioural factors. Biologically, men exhibit higher expression of ACE2 receptors and possess relatively weaker immune responses than women, possibly due to the immunomodulatory advantage conferred by the second X chromosome in females. Behavioural factors such as greater occupational exposure, higher tobacco and alcohol use, and reduced healthcare-seeking behaviour may further contribute to increased severity among males.25,26
Our findings showed a significant correlation between BMI and the severity of disease, indicated by the category of infection (P = 0.006). Higher BMI was reported to increase the risk of severe COVID-19 outcomes, which include intensive care unit (ICU) admission, the requirement of mechanical ventilation and death.27,28 The severe outcomes observed in this group may be partly explained by the overexpression of ACE2 receptors in individuals with obesity, enabling increased infectivity by the virus.29 The elevated rate of viral entry then triggers the overstimulation of inflammatory mediators, thereby inducing chronic low-grade inflammation and possible manifestation of acute respiratory distress syndrome (ARDS).30,31 Despite this, obesity is not directly correlated with the antibody titre, with several studies suggesting that this condition negatively impacts the persistence of vaccine-induced immunity.32,33
Reinfections, confirmed through antigen-based rapid test kits (Ag-RTK), were observed in four participants during the study period. Although reinfection can serve as a natural booster, enhancing antibody production, this effect was not consistent across our cohort. Patients reinfected with the Delta variant showed variable antibody responses, whereas those who were infected with the Omicron variant have been associated with higher reinfection rates but possibly lower immunogenicity.34-36 As in other studies, the reinfections observed in this study did not result in severe outcomes, highlighting the potent protection afforded by hybrid immunity.37 It was assumed that these reinfections occurred possibly due to the Omicron variant, due to its domination during the timing of reinfection, although there was no evidence to support this.
Our findings demonstrated the persistence of anti-SARS-CoV-2 IgG antibodies up to 390 days post-infection and post-vaccination, reaffirming the relevance of serological assays in monitoring convalescent-phase immunity. Long-lasting seropositivity has been previously reported for other coronaviruses, including MERS-CoV, with IgG detectable for up to four years.38 Among participants who received two vaccine doses, the data analysis demonstrated a negative correlation between antibody titre and time since vaccination, indicating a gradual decline in IgG levels over time. This observation is consistent with global studies reporting waning antibody levels following the primary series of vaccination.21,39,40 Conversely, participants who received a third (booster) dose exhibited more stable and higher antibody titres over time. This trend supports findings from studies in Japan, which demonstrated prolonged antibody persistence following booster vaccination.13,41 It is plausible that some participants sampled early post-booster had not yet reached peak antibody levels, while those sampled later were already in the plateau phase of antibody persistence.
The severity of the initial infection also appeared to influence antibody levels. Participants with Category 5 infection, representing the most critical cases, recorded a higher mean antibody titre compared to those with Category 4. This finding is consistent with prior studies showing that patients with severe disease tend to develop stronger and longer-lasting antibody responses, possibly due to higher viral loads and more pronounced immune activation during acute illness.42-44 Moreover, individual variability in immune fitness may explain differing levels of antibody production among patients with similar disease categories.45,46
Neutralising antibodies (NAbs), which play a critical role in blocking viral entry into host cells, were assessed in this study using a surrogate virus neutralisation test (sVNT). The sVNT-based assay serves as a rapid and effective tool for anti-SARS-CoV-2 NAbs detection without the requirement of high-level biosafety facilities for conventional cell-based neutralisation tests.16,47 The high specificity and sensitivity of the platform in correlation with the traditional assay augment its robustness to be implemented in assessing the NAbs presence, which reflects the protective level following hybrid immunity.48,49 These antibodies were detectable in nearly all participants, except for one, who recorded the lowest IgG titre at the final visit (79.60 BAU/mL). Factors which may affect the production of this antibody include prolonged interval, coupled with the use of an inactivated virus vaccine, and co-morbidities which are known to impair immune responses.50-52
The type of vaccine administered also influenced antibody responses. Heterologous COVID-19 vaccination regimens, such as combining an inactivated vaccine like CoronaVac with an mRNA vaccine booster (e.g., BNT162b2), have been shown to elicit a stronger and broader immune response than homologous regimens.53-56 In our study, however, nearly all of the 24 participants received homologous vaccinations consisting entirely of CoronaVac, with only one participant receiving a heterologous regimen (CoronaVac followed by BNT162b2). Despite this, we observed a consistent trend of increasing IgG antibody titres following each booster dose over a one-year follow-up period, highlighting that even homologous regimens may provide sustained immune protection, particularly when multiple booster doses are administered. When comparing types of vaccinations, the inactivated vaccine was reported to induce a less robust humoral immune response than the other strategies due to the non-replicative nature of the attenuated pathogens, which limits the magnitude and duration.57,58 In addition, the presentation of a wide array of antigens on the attenuated viral surface triggers a broad-spectrum antibody response or polyclonal antibody production, not mainly targeting the spike. This reduces the production of neutralising anti-spike antibodies, which is being assessed as the indication of protection and neutralising capacity in this study.59,60 With the low number of participants, this study is unable to assess the correlation between the type of vaccination and the dynamics and longevity of the anti-SARS-CoV-2 antibody titres.
Although 266.7 ± 30.9 BAU/mL was the highest titre measured in our cohort, this value is still lower than antibody levels typically reported or expected elsewhere. For instance, Lau et al. and Nanda et al. reported median titres exceeding 1,000 BAU/mL and 285 BAU/mL following mRNA-based and viral vector platforms, respectively.60,61 In another study, SinoVac or inactivated virus-based vaccine recipients recorded a median IgG titre of 214.50 BAU/mL at week 16 following vaccinations.62 Despite this relatively low mean antibody titre in our cohort, nearly all participants except one demonstrated the presence of neutralising antibodies (NAbs), suggesting functional immune protection. This finding underscores that IgG titres alone, particularly those targeting only the RBD, may not fully reflect the protective immunity against SARS-CoV-2. Previous research has shown that neutralising and protective antibodies can also target other spike protein domains, such as the N-terminal domain (NTD), and even non-spike viral antigens.7,63,64 Hence, the inclusion of additional antigenic targets in antibody assessments may provide a more accurate picture of immune protection, beyond the measured RBD-specific IgG levels.
This study had several limitations. First, we lacked a control group comprising individuals with purely vaccine-induced or natural infection-induced immunity, which limited our ability to isolate the effects of each exposure type. Second, the lack of comprehensive data on the exact vaccine types and dates for each participant hindered detailed vaccine-specific analysis. Third, the interval between vaccination and antibody measurement varied considerably among participants, which may have influenced the observed antibody titres, as antibody levels decline over time following COVID-19 vaccination.61,62
Next, our small sample size and focus on patients attending follow-up at a respiratory clinic reduce the generalisability of the findings to the broader population. Additionally, the variable timing of blood sample collection post-vaccination or infection may have introduced heterogeneity in observed antibody levels. While this study focused on assessing the longitudinal antibody dynamics following hybrid immunity, the small number of participants receiving heterologous vaccinations limits our ability to draw accurate conclusions on the effectiveness of heterologous vaccinations, despite supportive clinical evidence in various studies.
Nonetheless, this study provides valuable insights into the durability and variability of humoral immune responses following hybrid immunity in a real-world clinical cohort. The hybrid immunity, conferred through both infection and vaccination, appeared to result in more sustained IgG and NAbs responses. However, responses varied depending on age, sex, comorbidities, timing of vaccination, and vaccine type.
Future research should include larger and more diverse cohorts to better understand the long-term durability and breadth of hybrid immunity, especially against emerging SARS-CoV-2 variants. Investigating the therapeutic potential of hybrid-induced antibodies and their role in post-COVID-19 recovery syndromes would further enhance our understanding of protective immunity. Such findings may inform future vaccination policies, optimise the timing and composition of booster programmes, and contribute to more effective pandemic preparedness and response strategies.
This study highlights the important role of booster doses in extending the longevity of the antibody produced through hybrid immunity, primarily obtained through infection and primary vaccinations. However, relying solely on anti-RBD levels may not accurately reflect overall immunity, as neutralising antibodies, which may target other antigenic determinants, act as the key indicators of protection against infection and severe disease. In light of this, as supported by several studies, heterologous vaccination, especially with an mRNA booster in addition to the primary doses of inactivated vaccines, is recommended for a more durable and longer-lasting immunity.
ACKNOWLEDGMENTS
None.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
FUNDING
This study was funded by the Faculty of Medicine, Universiti Teknologi MARA, through GPM grant 600-RMC 5/3/GPM (034/2022).
DATA AVAILABILITY
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
ETHICS STATEMENT
This study was conducted in compliance with the tenets of the Helsinki Declaration and approved by the Research Ethics Committee (REC), Universiti Teknologi MARA (Reference No. REC/08/2021 FB/49).
INFORMED CONSENT
Written informed consent was obtained from the participants before enrolling in the study.
- Hamrouni AM, Sharif RS, Sharif SI, Hassanein MM, Abduelkarem AR. Impacts of COVID-19 pandemic on geopolitics, health, economics, education and sociocultural events. Risk Manag Healthc Policy. 2022;15:935-943.
Crossref - Ghebreyesus TA. WHO Director-General’s opening remarks at the media briefing on COVID-19 – 3 March 2020. World Health Organization. March 3, 2020. Accessed July 31, 2024. https://www.who.int/news-room/speeches/item/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—3-march-2020
- World Health Organization. WHO COVID-19 dashboard. Accessed December 18, 2025. https://covid19.who.int
- Annex 2m: Guideline on home monitoring and management of confirmed COVID-19 cases at CAC in primary care (3rd rev). https://covid-19.moh.gov.my, Accessed August 20, 2024.
- Centers for Disease Control and Prevention. People with certain medical conditions. Accessed March 27, 2026. https://www.cdc.gov/covid/risk-factors/index.html
- World Health Organization. COVID-19 advice for the public: Getting vaccinated. Updated October 8, 2024. Accessed August 5, 2023 https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines/advice
- Chen Y, Zhao X, Zhou H, Zhu H, Jiang S, Wang P. Broadly neutralizing antibodies to SARS-CoV-2 and other human coronaviruses. Nat Rev Immunol. 2023;23(3):189-199.
Crossref - Jafari M, Asli S, Moghbeli F, et al. Persistence of SARS-CoV-2 antibodies against N, S, and RBD after natural infection. Iran J Microbiol. 2023;15(6):803-810.
Crossref - Lugo-Trampe A, Lopez-Cifuentes D, Mendoza-Perez P, et al. Nine-month trend of IgG antibody persistence and associated symptoms post–SARS-CoV-2 infection. Healthcare. 2024;12(9):948.
Crossref - Al-Tamimi M, Tarifi AA, Qaqish A, et al. Immunoglobulin responses of COVID-19 patients, COVID-19 vaccine recipients, and random individuals. PLoS One. 2023;18(2):e0281689.
Crossref - Carvalho A, Henriques AR, Queiros P, et al. Persistence of IgG COVID-19 antibodies: a longitudinal analysis. Front Public Health. 2022;10:1069898.
Crossref - Pagheh AS, Ziaee A, Abrari Romenjan K, et al. SARS-CoV-2 IgG-specific antibody persistence in recovered COVID-19 individuals and its association with severity and time of illness. New Microbes New Infect. 2023;52:101096.
Crossref - Kusunoki H, Ekawa K, Ekawa M, et al. Trends in antibody titers after SARS-CoV-2 vaccination: insights from self-paid tests at a general internal medicine clinic. Medicines. 2023;10(4):27.
Crossref - Park JH, Cha MJ, Choi H, et al. Relationship between SARS-CoV-2 antibody titer and the severity of COVID-19. J Microbiol Immunol Infect. 2022;55(6 Pt 1):1094-1100.
Crossref - Li CJ, Chang SC. SARS-CoV-2 spike S2-specific neutralizing antibodies. Emerg Microbes Infect. 2023;12(2):2220582.
Crossref - Nkinda L, Shayo V, Masoud S, et al. Evaluation of a surrogate virus neutralization assay for detecting neutralizing antibodies against SARS-CoV-2 in an African population. Biol Methods Protoc. 2025;10(1):bpae095.
Crossref - Chemaitelly H, Ayoub HH, Coyle P, et al. Differential protection against SARS-CoV-2 reinfection pre- and post-Omicron. Nature. 2025;639(8056):1024-1031.
Crossref - Sarkar M, Madabhavi I. COVID-19 mutations: an overview. World J Methodol. 2024;14(3):89761.
Crossref - Shukri AMA, Wang SM, Chia SL, Nawi SFAM. The SARS-CoV-2 variants and their impacts. J Pure Appl Microbiol. 2022;16(3):1409-1424.
Crossref - Fewtrell MS, Kennedy K, Singhal A, et al. How much loss to follow-up is acceptable in long-term randomised trials and prospective studies? Arch Dis Child. 2008;93(6):458-461.
Crossref - Haq MA, Roy AK, Ahmed R, et al. Antibody longevity and waning following COVID-19 vaccination in a 1-year longitudinal cohort in Bangladesh. Sci Rep. 2024;14(1):11467.
Crossref - Caruana EJ, Roman M, Hernandez-Sanchez J, Solli P. Longitudinal studies. J Thorac Dis. 2015;7(11):E537-E540.
Crossref - Sieurin J, Branden G, Magnusson C, Hergens MP, Kosidou K. A population-based cohort study of sex and risk of severe outcomes in COVID-19. Eur J Epidemiol. 2022;37(11):1159-1169.
Crossref - Twitchell DK, Christensen MB, Hackett G, Morgentaler A, Saad F, Pastuszak AW. Examining male predominance of severe COVID-19 outcomes: a systematic review. Androg Clin Res Ther. 2022;3(1):41-53.
Crossref - Borges J, Byrne M. Investigating COVID-19 risk perception and preventive behaviours in third-level students in Ireland. Acta Psychol. 2022;224:103535.
Crossref - Bwire GM. Coronavirus: why men are more vulnerable to COVID-19 than women? SN Compr Clin Med. 2020;2(7):874-876.
Crossref - Singh R, Rathore SS, Khan H, et al. Association of obesity with COVID-19 severity and mortality: an updated systematic review, meta-analysis, and meta-regression. Front Endocrinol. 2022;13:780872.
Crossref - Mahamat-Saleh Y, Fiolet T, Rebeaud ME, et al. Diabetes, hypertension, body mass index, smoking and COVID-19–related mortality: a systematic review and meta-analysis of observational studies. BMJ Open. 2021;11(10):e052777.
Crossref - Yang Y, Song Y, Hou D. Obesity and COVID-19 pandemics: epidemiology, mechanisms, and management. Diabetes Metab Syndr Obes. 2023;16:4147-4156.
Crossref - Lippi G, Mattiuzzi C, Sanchis-Gomar F. COVID-19 and obesity: 2025 perspective on epidemiology, pathogenesis, and public health implications. J Lab Precis Med. 2025;10:10137.
- Montazersaheb S, Khatibi SMH, Hejazi M, et al. COVID-19 infection: an overview on cytokine storm and related interventions. Virol J. 2022;19:92.
Crossref - Chauvin C, Retnakumar SV, Bayry J. Obesity negatively impacts maintenance of antibody response to COVID-19 vaccines. Cell Rep Med. 2023;4(7):101117.
Crossref - Faizo AA, Qashqari FS, El-Kafrawy SA, et al. A potential association between obesity and reduced effectiveness of COVID-19 vaccine–induced neutralizing humoral immunity. J Med Virol. 2023;95(1):e28130.
Crossref - Ozudogru O, Bahce YG, Acer O. SARS-CoV-2 reinfection rate is higher in the Omicron variant than in the Alpha and Delta variants. Ir J Med Sci. 2023;192(2):751-756.
Crossref - Md Iderus NH, Lakha Singh SS, Mohd Ghazali S, et al. Correlation between population density and COVID-19 cases during the third wave in Malaysia: effect of the Delta variant. Int J Environ Res Public Health. 2022;19(12):7439.
Crossref - Yang SL, Teh HS, Suah JL, Husin M, Hwong WY. SARS-CoV-2 in Malaysia: a surge of reinfection during the predominantly Omicron period. Lancet Reg Health West Pac. 2022;26:100572.
Crossref - Bobrovitz N, Ware H, Ma X, et al. Protective effectiveness of previous SARS-CoV-2 infection and hybrid immunity against the Omicron variant and severe disease: a systematic review and meta-regression. Lancet Infect Dis. 2023;23(5):556-567.
Crossref - Cheon S, Park U, Park H, et al. Longevity of seropositivity and neutralizing antibodies in recovered MERS patients: a 5-year follow-up study. Clin Microbiol Infect. 2022;28(2):292-296.
Crossref - Hoeve CE, Huiberts AJ, de Gier B, et al. COVID-19 vaccination–induced antibody responses and waning by age and comorbidity status in a large population-based prospective cohort study. Vaccine. 2024;42(25):126121.
Crossref - Anastassopoulou C, Antoni D, Manoussopoulos Y, et al. Age and sex associations of SARS-CoV-2 antibody responses post BNT162b2 vaccination in healthcare workers: A mixed effects model across two vaccination periods. PLoS One. 2022;17(4):e0266958.
Crossref - Gilboa M, Regev-Yochay G, Mandelboim M, et al. Durability of immune response after COVID-19 booster vaccination and association with Omicron infection. JAMA Netw Open. 2022;5(9):e2231778.
Crossref - Movsisyan M, Truzyan N, Kasparova I, et al. Tracking the evolution of anti–SARS-CoV-2 antibodies and long-term humoral immunity within 2 years after COVID-19 infection. Sci Rep. 2024;14(1):13417.
Crossref - Yang G, Cao J, Qin J, et al. Initial COVID-19 severity influenced by SARS-CoV-2–specific T cells imprints T-cell memory and inversely affects reinfection. Signal Transduct Target Ther. 2024;9(1):141.
Crossref - Imai K, Kitagawa Y, Tabata S, et al. Antibody response patterns in COVID-19 patients with different levels of disease severity in Japan. J Med Virol. 2021;93(5):3211-3218.
Crossref - Vagts CL, Chang YS, Ascoli C, et al. Trimer IgG and neutralising antibody response to COVID-19 mRNA vaccination in individuals with sarcoidosis. ERJ Open Res. 2023;9(1):00025-2022.
Crossref - Ahmed S, Mehta P, Paul A, et al. Postvaccination antibody titres predict protection against COVID-19 in patients with autoimmune diseases: survival analysis in a prospective cohort. Ann Rheum Dis. 2022;81(6):868-874.
Crossref - Santos da Silva E, Servais JY, Kohnen M, et al. Validation of a SARS-CoV-2 surrogate neutralization test detecting neutralizing antibodies against major variants of concern. Int J Mol Sci. 2023;24(19):14965.
Crossref - Ali DW, Bartlett ML, Heger CD, et al. Automated and virus variant–programmable surrogate test qualitatively compares to the gold standard SARS-CoV-2 neutralization assay. Npj Viruses. 2024;2(1):83.
Crossref - Pieri M, Infantino M, Manfredi M, et al. Performance evaluation of four surrogate virus neutralization tests in comparison to the in vivo gold standard test. Front Biosci. 2022;27(2):74.
Crossref - Li J, Nakagawa T, Kojima M, et al. Underlying medical conditions and anti-SARS-CoV-2 spike IgG antibody titers after two doses of BNT162b2 vaccination: A cross-sectional study. PLoS One. 2023;18(4):e0283658.
Crossref - Soegiarto G, Wulandari L, Purnomosari D, et al. Hypertension is associated with antibody response and breakthrough infection in healthcare workers following vaccination with inactivated SARS-CoV-2. Vaccine. 2022;40(30):4046-4056.
Crossref - Lampasona V, Secchi M, Scavini M, et al. Antibody response to multiple antigens of SARS-CoV-2 in patients with diabetes: an observational cohort study. Diabetologia. 2020;63(12):2548-2558.
Crossref - Ann Costa Clemens S, Weckx L, Milan EP, Smolenov I, Clemens R. Interchangeability of different COVID-19 vaccine platforms as booster doses: A phase 3 study mimicking real-world practice. Vaccine. 2024;42(19):3989-3998.
Crossref - Ng HM, Lei CL, Fu S, et al. Heterologous vaccination with inactivated vaccine and mRNA vaccine augments antibodies against both spike and nucleocapsid proteins of SARS-CoV-2: a local study in Macao. Front Immunol. 2023;14:1131985.
Crossref - Zhang X, Xia J, Jin L, et al. Effectiveness of homologous or heterologous immunization regimens against SARS-CoV-2 after two doses of inactivated COVID-19 vaccine: A systematic review and meta-analysis. Hum Vaccin Immunother. 2023;19(2):2221146.
Crossref - Saltoğlu N, Dinç HÖ, Balkan İİ, et al. Heterologous booster COVID-19 vaccination elicited potent immune responses in HCWs. Diagn Microbiol Infect Dis. 2022;104(2):115758.
Crossref - Liu Y, Wang Z, Zhuang X, et al. Inactivated vaccine–elicited potent antibodies broadly neutralize circulating SARS-CoV-2 variants. Nat Commun. 2023;14(1):2179.
Crossref - Kan AKC, Li PH. Inactivated COVID-19 vaccines: potential concerns of antibody-dependent enhancement and original antigenic sin. Immunol Lett. 2023;259:21-23.
Crossref - Yang L, Xu L, Guo Q, et al. Immune responses to inactivated COVID-19 vaccine were decreased in Chinese patients with chronic respiratory diseases. Int J Med Sci. 2023;20(6):737-748.
Crossref - Lau JFW, Woon YL, Leong CT, Teh HS. Factors influencing acceptance of the COVID-19 vaccine in Malaysia: a web-based survey. Osong Public Health Res Perspect. 2021;12(6):361-373.
Crossref - Nanda R, Gupta P, Giri AK, Patel S, Shah S, Mohapatra E. Serological evaluation of antibody titers after vaccination against COVID-19 in 18–44-year-old individuals at a tertiary care center. Cureus. 2023;15(6):e40543.
Crossref - Tan CS, Noni V, Melina WUHU, et al. Antibody dynamics post-Comirnaty and CoronaVac vaccination in Malaysia. Sci Rep. 2022;12(1):15665.
Crossref - Garrido JL, Medina MA, Bravo F, et al. IgG targeting distinct seasonal coronavirus–conserved SARS-CoV-2 spike subdomains correlates with differential COVID-19 disease outcomes. Cell Rep. 2022;39(9):110904.
Crossref - Voss WN, Hou YJ, Johnson NV, et al. Prevalent, protective, and convergent IgG recognition of SARS-CoV-2 non-RBD spike epitopes. Science. 2021;372(6546):1108-1112.
Crossref
© The Author(s) 2026. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.