


ISSN: 0973-7510
E-ISSN: 2581-690X
The world experienced the outbreak of a new pandemic disease in 2019, known as coronavirus (CoV) disease 2019 (COVID-19), which is caused by the novel severe acute respiratory syndrome-CoV-2 (SARS-CoV-2). The respiratory system is the organ system most commonly affected by COVID-19; however, several other organ systems have been reported to be affected. The SARS-CoV-2 RNA found in infected stub samples can cause lung contagion by binding to the angiotensin-converting enzyme-2 (ACE-2) receptor of the alveolar epithelial cells. The gut microbiota (GM) promote immunity, indicating that the alignment of the microbiota and corresponding metabolic processes in COVID-19 can help to identify novel biomarkers and new therapeutic targets for this disease. The cause of kidney damage in COVID-19 patients is possibly multifactorial, involving a complex mechanism that involves complement dysregulation and thrombotic microangiopathy, as well as the occurrence of a “cytokine storm” syndrome, which are immune responses that are abandoned and dysfunctional with unfavorable prognosis in severe COVID-19 cases. Furthermore, COVID-19 involves a continuous proliferation and activation of macrophages and lymphocytes. SARS-CoV-2 can also bind to the ACE-2 receptor expressed in the cerebral capillary endothelial cells that can invade the blood-brain wall, to penetrate the brain parenchyma. However, in the ongoing pandemic, there has been a surge in studies on a wide range of topics, including causes of respiratory failure, asymptomatic patients, intensive care patients, and survivors. This review briefly describes the damaging effects of COVID-19 on vital human organs and the inhibitory function of the ACE-2 receptor on the GM, which causes gut dysbiosis, and thus, this review discusses topics that have an opportunity for further investigation.
COVID-19, SARS-CoV-2, ACE-2, Gut microbiome, Body organs
Currently, coronavirus (CoV) disease-2019 (COVID-19) is a public health concern due to its rapid spread and high mortality rate throughout the world, despite its discovery in late 2019 in Wuhan, the capital of the Hubei province of China1. The causative agent of COVID-19 is severe acute respiratory syndrome-CoV-2 (SARS-CoV-2)2. In January 2020, a study reported that RNA detected in COVID-19 patients was similar to the SARS-CoV-2 viral genome responsible for causing bilateral interstitial pneumonia2. This virus is included in the β-CoV cluster of viruses that causes SARS and Middle East respiratory syndrome (MERS), based on a report by the World Health Organization (WHO)2-5. The symptoms of COVID-19, including shortness of breath, fever, coughing, and pneumonia, typically appear between 2 and 14 days after the viral infection. Moreover, it can harm other organs in the body, such as the intestines, liver, and brain, as well as cause lung-related problems after hospitalization, which may ultimately lead to rapid death compared to those observed in previous cases of SARS- and MERS-CoV infections6-8. Recently, different research teams have been trying to develop novel SARS-CoV-2 therapies or vaccines and new solutions to prevent or halt the replication of the virus. In addition to the vaccine development efforts, multiple therapy options, including the use of drugs for blocking the ACE-2 receptor found in human cells, are currently being assessed9-12. Furthermore, ACE-2 also demonstrates anti-renin-angiotensin system (RAS) functions associated with the carriage of neutral amino acids and healthy homeostasis13,14. It is also associated with gastrointestinal (GI) symptoms such as diarrhoea and nausea15. Mounting evidence suggest that ACE-2 plays a vital role in the progression of gut dysbiosis in response to renal, metabolic, and cardiovascular distress associated with older age16-19. Moreover, there is an increased risk of multi-organ failure with an increasing death rate in the elderly COVID-19 patients with prevailing renal, metabolic, and cardiovascular conditions. Therefore, the disease incidences and mortality rates are much higher for the elderly population20-22. Acute kidney injury (AKI) is a condition where in the glomerular filtration rate unexpectedly decreases with nitrogen waste retention, along with affecting the fluid content, electrolytes, and homeostasis23,24. The WHO earlier declared that currently, there is no specific treatment or vaccine for COVID-1925; however, human clinical trials with few vaccines have already been started in many countries. In this review, we aimed to describe the damaging effects of COVID-19 on vital body organs of individuals with age-related comorbidities, as well as to explore the interactive role of intestinal microbiota dysbiosis in individuals with mutant ACE-2 receptors.
Table (1):
List of body parts affected by COVID-19 and its deleterious effects .
| Body organs/parts | Acts on/ Type of cell affected | Damage/Consequences | References |
|---|---|---|---|
| Gut Microbiota | Decrease probiotic microorganisms | Gut dysbiosis | 30, 31 |
| Small intestine, enterocytes, colon | Inflammation and diarrhea | 32 | |
| Kidney | Podocytes and proximally straight tubular cells | Acute Kidney Injury (AKI) | 33 |
| Glomerular cells, tubular epithelium, and podocytes | Rhabdomyolysis, hypoxemia, and coagulopathy | 34 | |
| Liver | Cells of the bile duct | Irregular liver function | 35, 36 |
| Heart | Pericytes | Microvascular disorders | 36 |
| Myocardium | Myocarditis | 37 | |
| Endothelial cells | Acute Coronary Syndrome | 38 | |
| Lungs | Alveolar cell | Alveolar damage, hypoxemia | 39 |
| Hyper fusion of alveolar cells | Acute Respiratory Distress Syndrome | 40 | |
| Brain | ACE-2 receptor affected due to amplified blood pressure | Cerebral hemorrhage | 41 |
| Neuronal destruction and nerve tissue lesions | Encephalitis | 42 | |
| Cerebral capillary endothelial cells | Puzzlement, loss of awareness, coma | 43 |
Organs affected by COVID-19
SARS-CoV-2 infection impacts different parts of the human body, including the gut microbiota (GM), heart, lungs, liver, brain, and kidneys, causing acute to severe damage. Table 1 presents the list of different body parts affected by COVID-19 and its deleterious effects on them; major effects of COVID-19 on the human body are depicted in Fig. 1.

Fig 1. Effects of COVID-19 on major parts of the human body.
Gut microbiota
The number of resident microorganisms in the human GM approximately exceeds 1014 and includes fungi, viruses, archaea, and bacteria5. Zuo et al. found significant alterations in fecal microbiomes of COVID-19 patients compared to those of healthy and pneumonia controls, after adjusting for age, gender, antibiotic use, and comorbidities26. The GM plays an important role in human health through its metabolic, nutritional, and defensive functions. Firmicutes and Bacteroidetes cause gut dysbiosis, while Firmicutes, Proteobacteria, and Bacteroidetes dominate throughout the lungs27. Previous studies have suggested variations in GM due to respiratory infections28. Pneumonia is a severe clinical symptom of COVID-19, which can cause acute respiratory distress syndrome (ARDS), specifically in elderly immune-compromised patients29.
GM and coronavirus infection
The GM plays a major role in host immunity by interacting with antigen-presenting cells. However, SARS-CoV-2 possibly interacts with the GM and infects enterocytes to induce GI symptoms. COVID-19 may interact with the microbiome and affect cytokine production, leading to the over-production of pro-inflammatory cytokines30. Previous studies, particularly on MERS- and SARS-CoV infections, have revealed that the resulting immune system “cytokine storm” was complimented by an impaired acute inflammatory reaction and the high expression of TNFα, IL-2, IL-6, IL-1β, MCP-1, IFNα, IFNβ, and IFNγ31,32. These findings are consistent with the high levels of pro-inflammatory cytokines (G-CSF, MIP-1A, IL-1, IL-2, IL-7, IP-10, TNFα, and MCP-1) in COVID-19 cases33. Based on these findings, new biomarkers are under investigation for the long-term improvement of the COVID-19 pandemic, considering the prevention of respiratory SARS-CoV-2 infections by age-linked pathways34. GM dysbiosis is characterized by a decrease in the levels of probiotic bacteria in COVID-19 patients due to imbalances in intestinal microflora35,36, relative abundance of pathogens (for example, Rothia, Actinomyces, and Streptococcus spp.), as well as interactions among pathogens37. These GM changes mainly occur following the resolution of respiratory symptoms and are correlated with the severity of COVID-1938. In general, these findings provide fundamental details of the research initiatives involving mammalian host immune interactions with the intestinal microbiota following SARS-CoV-2 infection39. Immunity against SARS-CoV-2 must be accurately evaluated under these circumstances, considering the effects of intestinal and lung microorganisms, as the host microbiome plays an essential role in infection.
GM permeability and dysbiosis in COVID-19 patients
A wide variety of age-related vascular and cardiac problems have been linked to GM, including heart failure, hypertension, coronary artery disease, myocardial infarction, and stroke18. The primary sign of specific strokes is a persistent inflammatory condition, which has also been linked to GM dysbiosis18,40. In kidney disease, immune deregulation and inflammation are both a cause and consequence of microbial dysbiosis41. Dysbiosis causes chronic inflammation and leads to renal disease, which ultimately modifies the GM, leading to dysbiosis42. Most medical conditions with a high mortality rate, caused due to SARS-CoV-2 infection, are related to increased intestinal dysbiosis, diabetes, obesity, lung inflammatory conditions, and cardiovascular disorders (CVDs)43. Furthermore, increased intestinal permeability is critical for viral infections because it is caused by initial inflammation (cytokine storm), thereby strengthening the previous fever44. As most viruses initially contact the host surfaces through bacteria, the interactions between bacteria and viruses are a long-standing element of viral pathophysiology45. Additionally, increased intestinal permeability contributes to higher TLR4 and lipopolysaccharide (LPS) levels46.
Crosstalk between GM and SARS-CoV-2
Robust biochemical and epidemiological findings during the COVID-19 pandemic indicate that older individuals with pre-existing lung, metabolic, cardiovascular, or renal infections are at a higher risk of severe sickness and death, upon SARS-CoV-2 infection47,48. The number of COVID-19 patients with diabetes, hypertension, or CVDs, receiving care at intensive care units (ICUs), is approximately two- to three-folds higher than that in a non-ICU treatment unit47. LPS-induced lung injury in rats decreases the expression of ACE-2, alleviating inflammation-related diseases and initiating the upregulation of Ras149. Notably, increasing of Ang II levels affects microbial gut metabolomics50. The gain and loss of ACE-2 function is associated with the improvement and deterioration of leaky intestinal conditions, respectively51. Enteric SARS-COV-2 infection and ACE2 imbalance, causing gastroenteritis-like symptoms, intestinal homeostasis disruption, and GM dysbiosis, are observed in COVID-19 patients52.
GM dysbiosis, altered intestinal permeability, and inefficient initiation of local and systemic immune responses can lead to severe symptoms because ACE-2 protective functions are lost upon SARS-CoV-2 infection53. For COVID-19 patients, GI impairment (for example, diarrhoea and GI discomfort) sustains until respiratory issues are mitigated15, which is similar to that observed in patients infected with other CoVs54. Abdominal pain is more prevalent in ICU-admitted patients than non-ICU admitted patients1. A pulmonary axis associated with phenotypic intestinal dysbiosis and permeable intestines, which corresponds to stimulation of the ACE/Ang II/AT1R axis, results from ACE-2 deficiency occurring at the onset of pulmonary hypertension55-57. The GM particularly causes pulmonary distress in a crucial cross-talk between itself and the lungs, called the “gut-lung axis”5. Some COVID-19 patients present with intestinal microbial dysbiosis, which supports this frame of logic35.
Effects of COVID-19 on the kidneys
It is essential to analyze the pathogenesis of COVID-19 to determine why renal failure can be a contributing factor in patients with SARS-CoV-2 infection. The development of an acute disease can be categorized into 3 distinct phases: an early infection phase, a pulmonary phase, and a severe hyper-inflammatory phase65,66,32. The ACE-2 receptor is expressed in various organs, including the kidneys53. ACE-2 and dipeptidyl peptidase-4, which can bind to SARS- and MERS-CoV, are expressed in renal tubular cells58,59. In both infections, viral RNA can be isolated via extraction from the kidneys and by collecting urine samples of the patients60. ACE-2 assists in viral entry by making the target cells vulnerable to some CoV, including SARS-CoV-261,62. A positive correlation exists between the expression of ACE-2 and SARS-CoV-2 in vitro. Thus, the expression of the human ACE-2 gene in various tissues may cause immune sensitization to SARS-CoV-2 infection21. Only 6% of SARS-CoV-2-infected subjects suffer from AKI63. Although AKI is a rare feature of SARS viral infection, it is a fatal complication; a high mortality rate has been observed in 5-15% of cases with AKI (60-90%). Expression of the ACE-2 and TMPRSS genes has been reported in cellular components of the kidney. In contrast, proximally straight tubular cells are potential SARS-CoV-2 hosts, with infections resulting in the development of AKI. In fatal pneumonia, synergistic cytopathic and systemic inflammatory attacks can affect AKI patients, particularly in serious and critical instances with positive viral RNA in blood and proteinuria64.
Renal impairment in COVID-19 patients
Researchers have analyzed the renal post-mortem viral nuclear capsid protein in situ and found that SARS-CoV-2 antigens aggregate in the kidney tubules, indicating that it specifically infects the human kidneys and causes AKI65. Alberici et al. identified 20 patients with kidney transplants and SARS-CoV-2-mediated pneumonia66. All the patients had fever, but only one had trouble breathing. With a median of 15 days post-symptom initiation, 5 kidney transplant recipients died, indicating rapid clinical deterioration and increased oxygen requirement in renal transplant patients with SARS-CoV-2 pneumonia. SARS-CoV-2-induced pneumonia had a high progression risk and a high mortality rate in this small cohort of long-term kidney transplant patients.
Uribarri et al. studied 758 patients, out of which 90.8% of the SARS-CoV-2-infected patients were identified through the nasopharyngeal PCR screening method67. Of these patients, 317 (48.9%) were diagnosed with hypertension, 290 (38.7%) with dyslipidemia, 138 (21.9%) with type-2 diabetes mellitus, 149 (19.5%) with pulmonary disorders, and 199 (26.0%) with cardiac disorders. However, only 8.5% of patients with a history of CKD showed kidney impairment, which was determined by measuring eGFR glomerular filtration rate after hospital admission. The patients received intensive COVID-19 medication. Systemic immunosuppression results in a poorer prognosis in organ transplantation patients with COVID-19 infection68. An intensive study by Wang et al. described the epidemiological and clinical characteristics of 138 patients with confirmed COVID-19-mediated pneumonia. The death rate was higher in patients with comorbidities, including ARDS1. Multisystem inflammatory syndrome in children (MIS-C) is a post-viral disease associated with COVID-19. However, it is still not known whether the AKI etiologies in MIS-C correlate with acute infections or whether the mechanisms are different for patients with a post-viral inflammatory condition.
Effects of COVID-19 on the liver
ACE2 has higher expression levels in the colon, liver, and biliary system35. ACE2 receptors are expressed in the gastrointestinal tract, vascular endothelium, and cholangiocytes of the liver. Therefore, cases of acute liver injury, having higher mortality associated with the effects of COVID-19, have been reported69. Previous studies have also reported that the subclinical features and laboratory test results of patients with COVID-19 infection are associated with liver dysfunction70. SARS-CoV-2 cannot cause viral hepatitis because of the low levels or a total lack of ACE-2 in hepatocytes. Generally, COVID-19 is correlated with mild-to-moderate levels of aspartate aminotransferase, and to a lesser degree, alanine aminotransferase elevations, with elevated aminotransferase levels more common in patients with mild disease than in those with very mild disease33.
Alterations in the biochemistry of the liver upon COVID-19 infection include elevated levels of aminotransferase expression, with rare severe liver injuries and abnormalities in more severe cases of COVID-1933. Fever, dry cough, weakness, and troubled breathing are the primary signs of SARS-CoV-2 infection. Studies on liver function abnormalities have been previously reported46,48 and have identified ACE-2 receptor as the SARS-CoV-2 cell entrance receptor71. SARS-CoV-2 infection severity is correlated with the expression levels of IL-672. The use of various drugs such as antibiotics, antivirals, analgesics, and conventional Chinese medicine can cause liver damage in COVID-19 patients33. Currently, there is no robust evidence that liver damage during hospitalization of severe COVID-19 patients is fully drug-induced. A patient who died with COVID-19 after a liver operation displayed higher liver enzyme expression levels, possibly due to the fractional properties of the drugs, and liver dysfunction due to sepsis33. Hepatotoxicity in COVID-19 patients, caused due to viral hepatocyte-associated infection or drug toxicity, has also been reported. SARS-CoV-2 fixes cholangiocytes positive for ACE-2 and causes dysfunction73. COVID-19 causes a severe inflammatory reaction, which results in immune-mediated injury74. Significantly elevated levels of infection biomarkers such as CRP, LDH, D-dimer, serum ferritin, IL-6, and IL-2 were observed in acute COVID-1975. Patients with stable liver disease may be more susceptible to SARS-CoV-2-mediated liver injury76.
In COVID-19 patients, liver enzyme expression levels frequently increase, thereby indicating liver damage. Therefore, liver function is regularly and carefully monitored in COVID-19 patients, so that hepatitis, liver damage, and liver failure can be detected at early stages77. However, further investigation on the relationship between COVID-19 assessment and liver injury is required, as the liver damage mechanism for COVID-19 infection is still unknown and tends to be multifactorial78.
Effects of COVID-19 on the cardiovascular system
Acute infections of the respiratory system, including influenza, respiratory syncytial virus, and bacterial pneumonia, are the major causes of CVDs79. Some individuals develop extreme acute respiratory disorders as a result of SARS-CoV, MERS-CoV, or SARS-CoV-248. Cardiovascular problems may develop due to SARS-CoV infection, and myocardial infarction and acute coronary syndrome can occur after SARS80. SARS-CoV-2 appears to act on the middle region of the heart and cause myocarditis81. Myocardial injury is possibly associated with myocarditis and ischemia-related infections and is an important prognostic factor in COVID-19 cases82. Troponin, myoglobin, C-reactive protein, serum ferritin, and IL-6 expression levels were higher in patients who had died from COVID-19 than in those who had died of other reasons. COVID-19 patients have a high inflammatory load, which causes a spike in cardiac myocarditis-related diseases83. In a previous study, a novel CoV that uses ACE-2 inside cells, SARS-CoV, was detected in the heart. The study showed that SARS-CoV was capable of infecting the myocardium through the ACE-2 receptor in 35% of the subjects84. The liver synthesizes angiotensinogen, and the kidneys secrete renin; angiotensinogen and renin then produce angiotensin 1, which is secreted by the lungs. The direct invasion of cardiomyocytes by SARS-CoV-2 indicates malfunction in the cardiac tissue and appears symptom like minor inflammation in the heart and that it affects COVID-19 patients without significant myocardial injury45. COVID-19 infected death in hospital was significantly associated with age, inflammatory response, and cardiovascular comorbidities85. Patients who died from COVID-19 had a more significant proportion of both myocardial damage and related coronary comorbidities, indicating that heart complications typically coexist and evolve into permanent outcomes of underlying coronary diseases or risks86. Alternatively, pneumonia might increase the impact of inflammation in coronary atherosclerotic plaques through a systemic inflammatory reaction, rendering them unstable and vulnerable to rupturing82. Severe myocardial damage has been identified in COVID-19 patients. Interstitial mononuclear inflammatory infiltrates diffuse into the heart tissue in COVID-19 patients81, suggesting that COVID-19 is not explicitly involved in heart damage.
Effects of COVID-19 on the respiratory system
COVID-19 is mainly associated with the respiratory system. A genome-wide association study analyzed 8,582,968 single nucleotide polymorphisms in 1,980 patients from Italy and Spain and conducted a meta-analysis of the two case-control panels87. A gene cluster, 3p21.31, was identified as a susceptible locus in COVID-19 patients. In the meta-analysis, associations between rs11385942 at locus 3p21.31 and rs657152 at locus 9q34.2 were detected87. The study also confirmed the involvement of the ABO blood types. It was found that population with blood group A had a higher risk of COVID-19 infection than the other blood types, whereas blood group O provided a protective function compared to the other blood types87,88.
Majority of the COVID-19 patients in intensive care are hypoxemic, have characteristics of ARDS, and receive invasive mechanical ventilation89. Endotracheal intubation is avoided in severely hypoxemic patients90. Different COVID-19 symptoms are associated with ARDS. In a previous study, 8 patients showed hyperfusion in certain lung regions, particularly poorly ventilated ones. Blood gas analyses and CT scans revealed fractions of large shunts and minor gasless tissues91. The effects of SARS-CoV-2 on the heart and lungs are shown in Fig. 2.
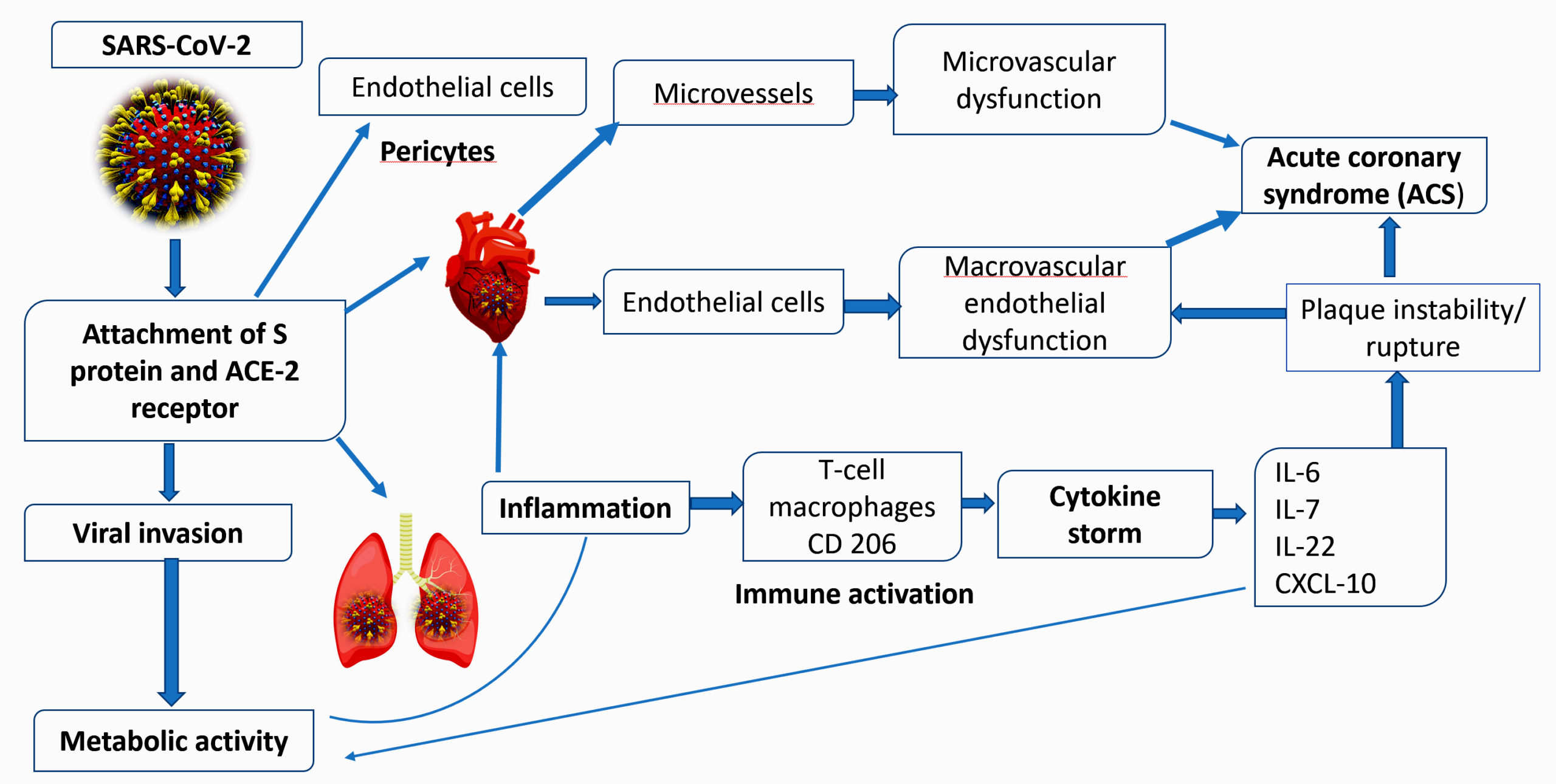
Fig 2. Effects of SARS-CoV-2 on the heart and lungs, which result in acute coronary syndrome (ACS).
The spike protein of SARS-CoV-2 first binds to the ACE-2 transmembrane receptor to enter the host cells, including endothelial cells and pericytes, leading to inflammation, and finally, to organ failure. The infection of endothelial cells or pericytes leads to severe microvascular and macrovascular dysfunction. In addition, it may effectively disrupt or rupture thrombotic plaques to develop acute coronary syndrome. SARS-CoV-2 infects the respiratory tract, particularly pneumocytes, and is characterized by the progression of systemic inflammation and overactivation of immune cells, resulting in a “cytokine storm,” i.e., an increased level of cytokines61.
Effects of COVID-19 on the brain
Initially, COVID-19 was thought to have influenza-like respiratory symptoms37. However, few neurological symptoms have been reported in patients with respiratory severities. SARS-CoV-2 infection is characterized by various signs and symptoms such as headaches, hemoptysis, diarrhoea, dyspnea, lymphopenia, and pneumonia with abnormalities in the chest CTs33, as well as cerebral hemorrhage, peripheral neuropathy, meningoencephalitis92, and cerebral infarction35. A recent study reported that more than one-third of 241 COVID-19 patients suffered several neurological disorders, including severe cerebrovascular disorders, skeletal muscle damage, and reduced consciousness92. Another study reported acute necrotizing encephalopathy from the brain MRIs of COVID-19 patients. Cerebral hemorrhage indicates that the ACE-2 receptors are affected by COVID-19 due to high blood pressure93.
Patients with severe infections may experience puzzlement, loss of awareness, and enter into a coma94,95. Nearly 40% of COVID-19 patients report increased depression, disturbed awareness, and other brain dysfunctions92. Additionally, an autopsy report showed brain tissue edema in a COVID-19 patient35.
ACE-2 expression is a brain-cardiac defense response in a variety of organs and organ systems, including the skeletal muscles and nervous system, and it plays a central role in regulating blood density and mechanisms of anti-atherosclerosis96. The brain expresses ACE-2 receptors in neurons and glial cells, making them a possible target of COVID-19. Previous studies have shown that SARS-CoV-2 can cause neuronal cell death in mice by penetrating the brain behind the nose near the olfactory epithelium97. A recent study by Mao et al. identified neurologic manifestations occurring in COVID-19 patients, indicating a prospective viral tropism in COVID-19 patients92. This indicates the prospective viral tropism of SARS-CoV-2.
A study published before the SARS-CoV-2 outbreak in the USA and Europe attempted to screen for ACE-2 mutants that could resist S-protein attachment. A recent study showed that the spike exterior glycoprotein (Ala930Val) in the Indian SARS-CoV-2 strain is different from that found in other strains98. Although cerebral damage in SARS-CoV-2-infected patients may be correlated with age and is predisposed in older patients, clinical trials have demonstrated that CoVs have tropism in the central nervous system99. Severe neurological disorders such as hemorrhages and acute necrotizing encephalopathy occur in COVID-19 patients because of the direct viral incursion into the nerve structure100,101.
In COVID-19 pathophysiology, ACE-2 has a series of functions that directly affect both disease treatment and outcome. The development of atherosclerosis and increased risk of death in patients with CVDs, obesity, diabetes, or chronic renal diseases, are strongly linked to microbiota dysbiosis and a compromised intestinal-blood barrier. In addition, gut dysbiosis in COVID-19 patients might be caused by AKI. Therefore, COVID-19 patients should undertake neurological examinations at an early stage, particularly for cerebrovascular infections, awareness, and paresthesia. However, there is still no specific cure for CoV infection. Therefore, primary intensive care is needed, which includes identifying critical signs, controlling blood pressure and oxygen, and treating and controlling other complications such as secondary infections and organ failure. Finally, analyzing the GM from the perspective of COVID-19 and exploring its modulation through probiotics, diet, and fecal transplants will provide insights into the interaction between the GM and SARS-CoV-2.
ACKNOWLEDGMENTS
The authors wish to thank Molecular Genetics Lab for all the support.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
MRC,MAM,MRA,MF,MFH, MNM developed the concept, involved in literature study and wrote the draft manuscript. MRA, MAI, ASS, MFH, MAH, MH and MMI revised the manuscript and assisted with literature search. MNM, MFH supervised the work and approved the manuscript for submission. All the authors carefully read the manuscript.
FUNDING
None.
ETHICS STATEMENT
Not applicable.
AVAILABILITY OF DATA
All datasets generated or analyzed during this study are included in the manuscript.
- Wang D, Hu B, Hu C, et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA. 2020;323(11):1061-1069.
Crossref - Wu Y, Guo C, Tang L, et al. Prolonged presence of SARS-CoV-2 viral RNA in faecal samples. Lancet Gastroenterol Hepatol. 2020;5(5):434-435.
Crossref - Perico L, Benigni A, Remuzzi G. Should COVID-19 Concern Nephrologists? Why and to What Extent? the Emerging Impasse of Angiotensin Blockade. Nephron. 2020;144(5):213-221.
Crossref - Chan JF-W, Yuan S, Kok K-H, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. The Lancet. 2020;395:514-523.
Crossref - Dhar D, Mohanty A. Gut microbiota and Covid-19- possible link and implications. Virus Res. 2020;285:198018.
Crossref - Meo SA, Alhowikan AM, Al-Khlaiwi T, et al. Novel coronavirus 2019-nCoV: Prevalence, biological and clinical characteristics comparison with SARS-CoV and MERS-CoV. Eur Rev Med Pharmacol Sci. 2020;24:2012-2019.
Crossref - Lai CC, Shih TP, Ko WC, Tang HJ, Hsueh PR. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int J Antimicrob Agents. 2020;55(3);105924.
Crossref - Siordia JA. Epidemiology and clinical features of COVID-19: A review of current literature. J Clin Virol. 2020;127:104357.
Crossref - Sanders JM, Monogue ML, Jodlowski TZ, Cutrell JB. Pharmacologic Treatments for Coronavirus Disease 2019 (COVID-19): A Review. JAMA. 2020;323(18):1824-1836.
Crossref - Li H, Liu SM, Yu XH, Tang SL, Tang CK. Coronavirus disease 2019 (COVID-19): current status and future perspectives. Int J Antimicrob Agents. 2020;55(5):105951.
Crossref - Zhang L, Liu Y. Potential interventions for novel coronavirus in China: A systematic review. J Med Virol. 2020;92(5):479-490.
Crossref - Shanmugaraj B, Siriwattananon K, Wangkanont K, Phoolcharoen W. Perspectives on monoclonal antibody therapy as potential therapeutic intervention for Coronavirus disease-19 (COVID-19). Asian Pacific J Allergy Immunol. 2020;38(1):10-18.
Crossref - Srivastava K. Association between COVID-19 and cardiovascular disease. Int J Cardiol Heart Vasc. 2020;29:100583.
Crossref - Perlot T, Penninger JM. ACE2 – From the renin-angiotensin system to gut microbiota and malnutrition. Microbes Infect. 2013;15(13):866-873.
Crossref - Kotfis K, Skonieczna-Zydecka K. COVID-19: Gastrointestinal symptoms and potential sources of SARS-CoV-2 transmission. Anaesthesiol Intensive Ther. 2020;52(2):171-172.
Crossref - Li Q, Guan X, Wu P, et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N Engl J Med. 2020;382(13):1199-1207.
Crossref - Mafra D, Borges N, Alvarenga L, et al. Dietary components that may influence the disturbed gut microbiota in chronic kidney disease. Nutrients. 2019;11(3):496.
Crossref - Sanchez-Rodriguez E, Egea-Zorrilla A, Plaza-Diaz J, et al. The gut microbiota and its implication in the development of atherosclerosis and related cardiovascular diseases. Nutrients. 2020;12(3):605.
Crossref - Abenavoli L, Scarpellini E, Colica C, et al. Gut microbiota and obesity: A role for probiotics. Nutrients. 2019;11(11):2690.
Crossref - Shi Q, Zhang X, Jiang F, et al. Clinical Characteristics and Risk Factors for Mortality of COVID-19 Patients with Diabetes in Wuhan, China: A Two-Center, Retrospective Study. Diabetes Care. 2020;43(7):1382-1391.
Crossref - Zhou F, Tu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. The Lancet. 2020;395(10229):1054-1062.
Crossref - Roncon L, Zuin M, Rigatelli G, Zuliani G. Diabetic patients with COVID-19 infection are at higher risk of ICU admission and poor short-term outcome. J Clin Virol. 2020;127:104354.
Crossref - Viana SD, Nunes S, Reis F. ACE2 imbalance as a key player for the poor outcomes in COVID-19 patients with age-related comorbidities – Role of gut microbiota dysbiosis. Ageing Res Rev. 2020;62:101123.
Crossref - Aleebrahim-Dehkordi E, Reyhanian A, Saberianpour S, Hasanpour-Dehkordi A. Acute kidney injury in COVID-19; A review on current knowledge. J Nephropathol. 2020;9(4):e31.
Crossref - Di Maira T, Berenguer M. COVID-19 and liver transplantation. Nat Rev Gastroenterol Hepatol. 2020;17(9):526-528.
Crossref - Zuo T, Zhang F, Lui GCY, et al. Alterations in Gut Microbiota of Patients With COVID-19 During Time of Hospitalization. Gastroenterology. 2020;159(3):944-955.e8.
Crossref - D Zhang, S Li, N Wang, HY Tan, Z Zhang, Y Feng. The Cross-Talk Between Gut Microbiota and Lungs in Common Lung Diseases. Front Microbiol. 2020;11:301.
Crossref - Groves HT, Higham SL, Moffatt MF, Cox MJ, Tregoning JS. Respiratory viral infection alters the gut microbiota by inducing inappetence. mBio. 2020;11(1):e03236.
Crossref - Lake MA. What we know so far: COVID-19 current clinical knowledge and research. Clin Med J R Coll Physicians London. 2020;20(2):124-127.
Crossref - Prompetchara E, Ketloy C, Palaga T. Immune responses in COVID-19 and potential vaccines: Lessons learned from SARS and MERS epidemic. Asian Pacific J Allergy Immunol. 2020;38(1):1-9.
Crossref - Jose RJ, Manuel A. COVID-19 cytokine storm: the interplay between inflammation and coagulation. Lancet Respir Med. 2020;8(6):e46-e47.
Crossref - Channappanavar R, Perlman S. Pathogenic human coronavirus infections: causes and consequences of cytokine storm and immunopathology. Semin Immunopathol. 2017;39(5):529-539.
Crossref - Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. The Lancet. 2020;395:497-506.
Crossref - Fuellen G, Liesenfeld O, Kowald A, et al. The preventive strategy for pandemics in the elderly is to collect in advance samples & data to counteract chronic inflammation (inflammaging). Ageing Res Rev. 2020;62:101091.
Crossref - Xu H, Zhong L, Deng J, et al. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int J Oral Sci. 2020;12.
Crossref - Guo YR, Cao QD, Hong ZS, et al. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak- An update on the status. Military Medical Research. 2020:7;11.
Crossref - Zhou P, Yang X-L, Wang X-G, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579(7798):270-273.
Crossref - Berta P, Siatka C, Le virus SARS-CoV-2 et la maladie COVID-19 : donnees moleculaires. Salles Propres. 2020;1-13.
- He Y, Wang J, Li F, Shi Y. Main Clinical Features of COVID-19 and Potential Prognostic and Therapeutic Value of the Microbiota in SARS-CoV-2 Infections. Front Microbiol. 2020;11:1302.
Crossref - Barrios C, Beaumont M, Pallister T, et al. Gut-microbiota-metabolite axis in early renal function decline. PLoS One. 2015;10(8):e0134311.
Crossref - Villena J, Kitazawa H. The Modulation of Mucosal Antiviral Immunity by Immunobiotics: Could They Offer Any Benefit in the SARS-CoV-2 Pandemic? Front Physiol. 2020;11:699.
Crossref - Sanada TJ, Hosomi K, Shoji H, et al. Gut microbiota modification suppresses the development of pulmonary arterial hypertension in an SU5416/hypoxia rat model. Pulm Circ. 2020;10(3).
Crossref - Anderson G, Maes M. Gut Dysbiosis Dysregulates Central and Systemic Homeostasis via Suboptimal Mitochondrial Function: Assessment, Treatment and Classification Implications. Curr Top Med Chem. 2020;20(7):524-539.
Crossref - Guan WJ, Ni ZY, Hu Y, et al. China medical treatment expert group for clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708-1720.
Crossref - Mehra MR, Desai SS, Kuy SR, Henry TD, Patel AN. Cardiovascular Disease, Drug Therapy, and Mortality in Covid-19. N Engl J Med. 2020;382:e102.
Crossref - Wang X, Fang X, Cai Z, et al. Comorbid Chronic Diseases and Acute Organ Injuries Are Strongly Correlated with Disease Severity and Mortality among COVID-19 Patients: A Systemic Review and Meta-Analysis. Research. 2020;2020:2402961
Crossref - Li M-Y, Li L, Zhang Y, Wang XS. Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infect Dis Poverty. 2020;9(1):45.
Crossref - Chen L, Li X, Chen M, Feng Y, Xiong C. The ACE2 expression in human heart indicates new potential mechanism of heart injury among patients infected with SARS-CoV-2. Cardiovasc Res. 2020;116(6):1097-1100.
Crossref - Sharma RK, Oliveira AC, Yang T, et al. Gut Pathology and Its Rescue by ACE2 (Angiotensin-Converting Enzyme 2) in Hypoxia-Induced Pulmonary Hypertension. Hypertension. 2020;76(5):e40.
Crossref - Cheema MU, Pluznick JL. Gut Microbiota Plays a Central Role to Modulate the Plasma and Fecal Metabolomes in Response to Angiotensin II. Hypertension. 2019;74(1):184-193.
Crossref - Duan Y, Prasad R, Feng D, et al. Bone Marrow-Derived Cells Restore Functional Integrity of the Gut Epithelial and Vascular Barriers in a Model of Diabetes and ACE2 Deficiency. Circ Res. 2019;125(11):969-988.
Crossref - Shi S, Qin M, Cai Y, et al. Characteristics and clinical significance of myocardial injury in patients with severe coronavirus disease 2019. Eur Heart J. 2020;41(22):2070-2079.
Crossref - Ye R, Liu Z. ACE2 exhibits protective effects against LPS-induced acute lung injury in mice by inhibiting the LPS-TLR4 pathway. Exp Mol Pathol. 2020;113:104350.
Crossref - Leung WK, To K-F, Chan PKS, et al. Enteric involvement of severe acute respiratory syndrome-associated coronavirus infection. Gastroenterology. 2003;125(4):1011-1017.
Crossref - Kim S, Rigatto, Gazzana MB, et al. Altered gut microbiome profile in patients with pulmonary arterial hypertension. Hypertension. 2020;75(4):1063-1071.
Crossref - Fu Y, Cheng Y, Wu Y. Understanding SARS-CoV-2-Mediated Inflammatory Responses: From Mechanisms to Potential Therapeutic Tools. Virol Sin. 2020;35(3):266-271.
Crossref - Siddiqi HK, Mehra MR. COVID-19 illness in native and immunosuppressed states: A clinical-therapeutic staging proposal. J Hear Lung Transplant. 2020;39(5):405-407.
Crossref - Fehr AR, Perlman S. Coronaviruses: An overview of their replication and pathogenesis. Methods Mol Biol. 2015;1282:1-23.
Crossref - Raj VS, Mou H, Smits SL, et al. Dipeptidyl peptidase 4 is a functional receptor for the emerging human coronavirus-EMC. Nature. 2013;495(7440):251-254.
Crossref - Peiris JSM, Chu CM, Cheng VCC, et al. Clinical progression and viral load in a community outbreak of coronavirus-associated SARS pneumonia: A prospective study. The Lancet. 2003;361(9371):1767-1772.
Crossref - Kuba K,Imai Y, Rao S, et al. A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus-induced lung injury. Nat Med. 2005;11(8):875-879.
Crossref - Zou L, Ruan F, Huan M, et al. SARS-CoV-2 Viral Load in Upper Respiratory Specimens of Infected Patients. N Engl J Med. 2020;382(12):1177-1179.
Crossref - Chu KH, Tsang WK, Tang CS, et al. Acute renal impairment in coronavirus-associated severe acute respiratory syndrome. Kidney Int. 2005;67(2):698-705.
Crossref - Cheng Y, Luo R, Wang X, et al. The incidence, risk factors, and prognosis of acute kidney injury in adult patients with coronavirus disease 2019. Clin J Am Soc Nephrol. 2020;15(10):1394-1402.
Crossref - Diao B, Wang C, Wang R, et al. Human Kidney is a Target for Novel Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). medRxiv. 2020.
Crossref - Alberici F, Delbarba e, Manenti C, et al. A single center observational study of the clinical characteristics and short-term outcome of 20 kidney transplant patients admitted for SARS-CoV2 pneumonia. Kidney Int. 2020;97(6):1083-1088.
Crossref - Uribarri A, Nunez-Gil IJ, Aparisi A, et al. Impact of renal function on admission in COVID-19 patients: an analysis of the international HOPE COVID-19 (Health Outcome Predictive Evaluation for COVID 19) Registry. J Nephrol. 2020;33(4):737-745.
Crossref - Zaki N, Alashwal H, Ibrahim S. Association of hypertension, diabetes, stroke, cancer, kidney disease, and high-cholesterol with COVID-19 disease severity and fatality: A systematic review. Diabetes Metab Syndr Clin Res Rev. 2020;14(5):1133-1142.
Crossref - Fan Z, Chen L, Li J, et al. Clinical Features of COVID-19-Related Liver Functional Abnormality. Clin Gastroenterol Hepatol. 2020;18(7):1561-1566.
Crossref - Jothimani D, Venugopal R, Abedin MF, Kaliamoorthy I, Rela M. COVID-19 and Liver. J Hepatol. 2020;73(5):1231-1240.
Crossref - Zou X, Chen K, Zou J, Han P, Hao J, han Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Front Med. 2020;14(2):185-192.
Crossref - Blanco-Melo D, Nilsson-Payan BE, Liu W-C, et al. Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19. Cell. 2020;181(5):1036-1045.e9.
Crossref - Zhang C, Shi L, Wang FS. Liver injury in COVID-19: management and challenges. The Lancet Gastroenterology and Hepatology. 2020;5(5):428-430.
Crossref - Mehta P, McAuley DF, Brown M, et al. COVID-19: consider cytokine storm syndromes and immunosuppression. The Lancet. 2020;395(10229):1033-1034.
Crossref - Liu W, Zhang Q, Chen J, et al. Detection of Covid-19 in Children in Early January 2020 in Wuhan, China. N Engl J Med. 2020;382(14):1370-1371.
Crossref - Mantovani A, Byrne CD, Zheng MH, Targher G. Diabetes as a risk factor for greater COVID-19 severity and in-hospital death: A meta-analysis of observational studies. Nutr Metab Cardiovasc Dis. 2020;30(8):1236-1248.
Crossref - Farshidpour M, Kim D, Junna S, Merchant J. A brief review of liver injury in patients with Corona Virus Disease-19 during the pandemic. Indian J Gastroenterol. 2020;39(3):232-235.
Crossref - Ali ST, Wang L, Lau EHY, et al. Serial interval of SARS-CoV-2 was shortened over time by nonpharmaceutical interventions. Science. 2020;369(6507):1106-1109.
Crossref - Cowan LT, Lutsey PL, Pankow JS, Matsushita K, Ishigami J, Lakshminarayan K. Inpatient and outpatient infection as a trigger of cardiovascular disease: The ARIC study. J Am Heart Assoc.2018;7:e009683.
Crossref - Chong PY, Chui P, Ling AE, et al. Analysis of Deaths during the Severe Acute Respiratory Syndrome (SARS) Epidemic in Singapore: Challenges in Determining a SARS Diagnosis. Arch Pathol Lab Med. 2004;128(2):195-204.
Crossref - Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8(4):420-422.
Crossref - Madjid M, Vela D, Khalili-Tabrizi H, Casscells SW, Litovsky S. Systemic infections cause exaggerated local inflammation in atherosclerotic coronary arteries: Clues to the triggering effect of acute infections on acute coronary syndromes. Texas Hear Inst J. 2007;34(1):11-18. PMID: 17420787
- Yang HJ, Zhang YM, Yang M, Huang X. Predictors of mortality for patients with COVID-19 pneumonia caused by SARS-CoV-2. Eur Respir J. 2020;56(3):2002439.
Crossref - Oudit GY, Kassiri Z, Jiang C, et al. SARS-coronavirus modulation of myocardial ACE2 expression and inflammation in patients with SARS. Eur J Clin Invest. 2009;39(7):618-625.
Crossref - Nishiga M, Cai Y, Liu T, et al. Characteristics and clinical significance of myocardial injury in patients with severe coronavirus disease 2019. Eur Heart J. 2020;41(22):2070-2079.
Crossref - Mancia G, Rea F, Ludergnani M, Apolone G, Corrao G. Renin-Angiotensin-Aldosterone System Blockers and the Risk of Covid-19. N Engl J Med. 2020;382(25):2431-2440.
Crossref - Group SC-19 G. Genomewide association study of severe Covid-19 with respiratory failure. N Engl J Med. 2020;383:1522-1534.
Crossref - Gorbalenya AE, Baker SC, Baric RS, et al. The species severe acute respiratory syndrome related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nat Microbiol. 2020;5:536-544.
Crossref - World Health Organization. Clinical management of severe acute respiratory infection (SARI) when COVID-19 disease is suspected: interim guidance. 2020:16(1);9-26.
Crossref - Villarreal-Fernandez E, Patel R, Golamari R, Khalid M, DeWaters A, Haouzi. A plea for avoiding systematic intubation in severely hypoxemic patients with COVID-19-associated respiratory failure. Crit Care. 2020;24(1):337.
Crossref - Fan E, beitler JR, Brochard L, et al. COVID-19-associated acute respiratory distress syndrome: is a different approach to management warranted? Lancet Respir Med. 2020;8(8):816-821.
Crossref - Mao L, Jin H, Wang M, et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 2020;77(6):683-690.
Crossref - Li YC, Bai WZ, Hashikawa T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J Med Virol. 2020:92(7):552-555.
Crossref - Dobbs MR. Toxic encephalopathy. Semin Neurol. 2011;31(2):184-193.
Crossref - Mizuguchi M, Yamanouchi H, Ichiyama T, Shiomi M. Acute encephalopathy associated with influenza and other viral infections. Acta Neurologica Scandinavica. 2007;115:45-56.
Crossref - Miller AJ, Arnold AC. The renin-angiotensin system in cardiovascular autonomic control: recent developments and clinical implications. Clin Auton Res. 2019;29:231-243.
Crossref - Netland J, Meyerholz DK, Moore S, Cassell M, Perlman S. Severe Acute Respiratory Syndrome Coronavirus Infection Causes Neuronal Death in the Absence of Encephalitis in Mice Transgenic for Human ACE2. J Virol. 2008;82(15):7264-7275.
Crossref - Sardar R, Satish D, Birla S, Gupta D. Integrative analyses of SARS-CoV-2 genomes from different geographical locations reveal unique features potentially consequential to host-virus interaction, pathogenesis and clues for novel therapies. Heliyon. 2020;6(9):e04658.
Crossref - Carod-Artal FJ. Neurological complications of coronavirus and COVID-19. Rev Neurol. 2020;70(9):311-322.
Crossref - Markus HS, Brainin M. COVID-19 and stroke-A global World Stroke Organization perspective. Int J Stroke. 2020;15(4):361-364.
Crossref - Sharifi-Razavi A, Karimi N, Rouhani N. COVID-19 and intracerebral haemorrhage: causative or coincidental? New Microbes New Infect. 2020;35:100669.
Crossref
© The Author(s) 2021. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.