

ISSN: 0973-7510
E-ISSN: 2581-690X
Mixed infections of enteric viruses and parasite can infected the human alimentary canal and quite complex physiological changes can result from such infection. To study the association between enteric viruses and giardiasis among diarrheal children as well as to clearly the relationship with Giardia lamblia genotypes in Diyala province, Iraq. Descriptive cross sectional study was conducted in Al-Batool Teaching Hospital for Maternity and Children in Baqubah city, during the period from June 2017 till November 2017. One hundred and sixty stool samples were collected from children with gastroenteritis using a clean and dry container. Samples, screened for rotavirus, adenovirus, astrovirus and norovirus using Cer Test Biotec, and G. lamblia by ELISA kits. The positive G. lamblia samples were further analyzed by nested polymerase chain reaction. Rotavirus was detected in 20%, adenovirus in 18.75% and norovirus in 13.75% while no positive result with astrovirus. G. lamblia were detected in 42 cases (26.25%), amplification triose phosphate isomerase (tpi) gene was successful in 28/42 (66.66%) samples, 8 (28.57%) contained genotype A and 20 (71.43%) samples contained genotype B. The majority of infected children were males less than five years old. Rotavirus infection rate amongst children in Diyala appears to be relatively higher than other enteric viruses. Co-infection with G. lamblia type B have important role.
Gastroenteritis, Enteric viruses, Giardia lamblia, Chromatographic Immunoassay
Gastroenteritis, which is also well-known as ‘infectious diarrhea’, is the inflammation that affect the stomach and small intestine of the digestive system1. Its signs and symptoms are a combination of diarrhea, vomiting, and abdominal pain2. Furthermore, fever, lack of energy, and dehydration could be occur in such cases3. By the end of 2015, there were about 1.3 million cases of gastroenteritis out of two billion ones who were reported to be dead4. Children and those in the developing counties are most commonly affected5. Risk of infection is higher in children due to their lack of immunity and relatively poor hygiene2. The disease is less common in adults, partly due to the development of immunity6.
Many microorganisms can cause gastroenteritis, such as: bacteria, parasites, fungus and viruses. However, viral gastroenteritis is regarded the most common one7. Rotavirus, norovirus, adenovirus, and astrovirus are known to cause viral gastroenteritis6. Rotavirus is the most common cause of gastroenteritis in children8, and produces similar rates in both the developed and developing world9. Many studies has concluded that viruses could be estimated as nearly 70% as the main reason behind the incidents of infectious diarrhea in the pediatric age of human beings10.
Likewise, gastroenteritis may be caused by a number of protozoa; most commonly G. lamblia. However, Entamoeba histolytica, Cryptosporidium spp. and other species have been additionally referred to in such related studies10. G. lamblia is the most common pathogenic intestinal parasite of humans worldwide and is a frequent cause of endemic and epidemic diarrhea. G. lamblia is divided into eight genotypes (A-H) which infect a wide range of mammals and humans, but human infections are caused by genotypes A and B11.
There is some evidence that clinical signs associated with assemblage A depend on the tpi gene target, Sahagun et al., demonstrated an association for G. lamblia assemblage A with gastroenteritis in children less than 5 years old12. Another study found the same correlation in children after assemblage typing analysis of the SSU-rRNA13. Whereas, others found a strong relationship with assemblage B14,15. Furthermore, one study showed that assemblage B exhibited more extensive association with persistent symptoms, while assemblage A was found in connection with intermittent diarrhea16. Most of the studies used one or two marker, and it is noticeable that the tpi gene was more often found to be associated with symptomatic assemblage A patients than the gdh and ²-giardin13.
Very few studies have been performed in Diyala province to determine the enteric pathogens and co-infection. To the best of our knowledge, there is no study about relationship between enteric viruses and G. lamblia genotypes. Hence, the current study was designed to assess this points.
Study design
This study was designed as descriptive cross sectional study and conducted in Al-Batool Teaching Hospital for Maternity and Children in Diyala province, Iraq during the period from July 2017 to November 2017.
Samples collection and processing
One hundred and sixty stool samples were collected from children with gastroenteritis using a clean and dry container. Age, gender and other demographic data were collected by direct interview with children’s parents.
Chromatographic immunoassay
Cer Test Rota-Adeno-Astro-Noro one step combo card test is a colored chromatographic immunoassay (Cer Test Biotic S.L, Zaragoza-Spain)[17]. It was used for the simultaneous qualitative detection of rotavirus, adenovirus, astrovirus and norovirus. This test is highly sensitive and specific to make a presumptive diagnosis of these viruses.
Enzyme immunoassay for the qualitative assessment of G. lamblia in fecal samples was done according to the (RIDASCREEN® Giardia test).
Extraction of G. lamblia DNA from Stool
The DNA extraction was performed by using AccuPrep® Genomic DNA extraction Kit (Cat No. K-3032-Korea) for stool according to the manufactures’ instructions. The extracted DNA was measured by Nano Drop 1000 spectrophotometer instrument and the purity was estimated with the OD260nm/OD280nm ratio, a ratio of 1.8 was generally accepted as pure for DNA. G. lamblia genotypes A identified by semi nested PCR through amplifying the tpi gene, for the first round of PCR, a PCR product of 605 bp was amplified by using primer set forward primer AL3543 and reverse primer AL3546 [18]. PCR mixture was prepared in 20 ¼l volume with 2 µl of extracted DNA in PCR master Mix (250 ¼M each of deoxynucleoside triphosphate (dNTP), {dATP, dTTP, dCTP, dGTP }, 1 U of Taq polymerase, 30 mM KCl, 1.5 mM MgCl2, 10 mM Tris-HCl, tracking dye and stabilizer), 1 ¼l of each of forward and reverser primer, 16 ¼l distilled water. The PCR conditions were as follows: – denaturation step: -95°C for 5 minutes 35 cycles: -94°C for 45 second -50°C for 45 second -72°C for 60 second -Final extension step: -72°C for 10 minutes. The second round of PCR was prepared as separate reactions for A [19] and B [20] genotype. Genotypes specific primers presence of mixed infection was detected by visualizing the occurrence of bands in the agarose gel 1.5%, at 332 bp for assemblage A amplified using primer sets forward primer AssAF and reverse primer AssAR and at 400 bp for genotype B, PCR amplification mixture was prepared in 20 ¼l final volume with 10 ¼l of the first round of PCR as a template DNA in master Mix (250¼M each of deoxynucleoside triphosphate (dNTP), {dATP, dTTP, dCTP, dGTP }, 1 U of Taq polymerase, 30 mM KCl, 1.5mM MgCl2, 10 mM Tris-HCl, tracking dye and stabilizer), 1 ¼l of each primer, 16 ¼l distilled water. The PCR conditions were as follows: – denaturation step: -94°C for 10 minutes -35 cycles: -94°C for 45 second -64°C for 45 second -72°C for 60 second -Final extension step: -72°C for 10 minutes. The PCR products were reorganized by electrophoresis in 1.5% agarose gel stained with 0.5 mg/ml ethidium bromide.
Data analysis
The Chi-square-X2 test and Fisher exact test were used to find out of different factors in study criteria; bellow or equal to (p d”0.05) was accepted as statistical significant difference.
The mean age of the 160 children infected with diarrhea was 4.53 year, range from (2 month- 15 year). The majority of diarrhea cases 108(67.50%) were observed in age group d”1-5 years than other groups; 52.50% were male and 47.50% were female, the result showed there was no gender significant preference to get the diarrhea as shown in (table 1).
Table (1):
Distribution of study group according to their age and gender
| Criteria | No. (%) | Comparison of Significance P-value Sig. |
|---|---|---|
| Age (years) | < 0.00001 * | |
| ≤1-5 years | 108(67.50%) | |
| 6-10 years | 38(23.75%) | |
| 11-15 years | 14(8.75%) | |
| Total | 160(100%) | |
| Gender | 0 .371** | |
| Males | 84(52.50%) | |
| Females | 76(47.50%) | |
| 160(100%) | ||
X2: Chi square, P: Probability,*Significant,**Non- significant.
Regarding enteric viruses infection, Cer Test one step detect 32 cases positive for rotavirus, 30 cases positive for adenovirus and 22 cases positive for norovirus while no positive cases with astrovirus as shown in table (2).
Table (2):
The intestinal viruses identified from study group by Cer Test one step
| Intestinal viruses | No. (%) | Comparison of Significance Chi2-value Sig. |
|---|---|---|
| Rotavirus | 32(20%) | < 0.00001 * |
| Adenovirus | 30(18.75%) | |
| Norovirus | 22(13.75%) | |
| Astrovirus | Zero | |
| Total | 160 |
* Significant
According to results of enzyme linked immunosorbant assay positive G. lamblia antigen was detected in 42 out of 160 cases (26.25%). Majority of infection among age group d”1-5 years also high percentage of infection was noticed in males 24/42 than females 18/42 as shown in table (3). And statistical analysis showed significant differences.
Table (3):
G. lamblia infection and related with age and gender in diarrheal children
| Criteria | No. (%) | Comparison of Significance P-value Sig. |
|---|---|---|
| Age (years) | 0.094 * | |
| ≤1-5 years | 34(80.95%) | |
| 6-10 years | 6(14.28%) | |
| 11-15 years | 2(4.77%) | |
| Total | 42(100%) | |
| Gender | 0.482 * | |
| Males | 24(57.15%) | |
| Females | 18(42.82%) | |
| 42(100%) | ||
* Non-Significant at p < 0.05
The results of tpi gene amplification has shown that G. lamblia was successful among 28/42 (66.66%) samples. Eight (28.57%) of samples were having genotype A (figure 1) while 20 (71.43%) of samples were having genotype B (figure 2). The distribution of genotypes among giardiasis patients in Diyala province was highly significant at Pd”0.001 as shown in table (4).
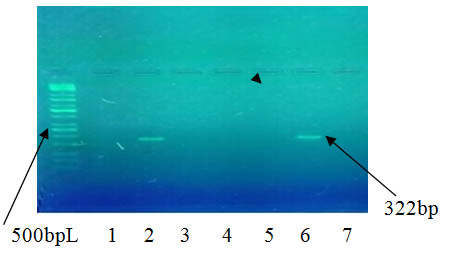
Fig. 1. G. lamblia genotyping A in agarose gel electrophoresis with an amplicon of 322bp (lanes 2,6). M: 100-10000 bp molecular marker. fragments were resolved on 1.5% agarose gel and visualized with red stain
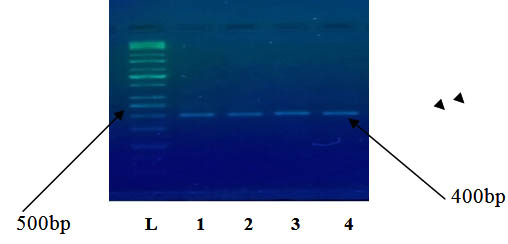
Fig. 2. G. lamblia genotyping B in agarose gel electrophoresis with an amplicon of 400bp (lanes 1-4). M: 100-10000 bp molecular marker. fragments were resolved on 1.5% agarose gel and visualized with red stain
Table (4):
Identification of G. lamblia genotypes by PCR technique
Genotypes |
No. of samples (%) |
|---|---|
A |
8 (28.57%) |
B |
20 (71.43%) |
Total |
28(100%) |
Significant P= 0.001
Regarding co-infection between G. lamblia and enteric viruses, high number (14 cases) was recorded with rotavirus followed by 6 cases with norovirus and 4 with adenovirus and statistically significant as shown in table (5).
Table (5):
Co-infection between G. lamblia and enteric viruses
G. lamblia |
Rotavirus |
Adenovirus |
Norovirus |
p-value |
|---|---|---|---|---|
G. lamblia – positive (42) |
14 |
4 |
6 |
0.013* |
G. lamblia – Negative (118) |
18 |
26 |
16 |
0.185** |
Total 160 |
32 |
30 |
22 |
0.297** |
P: Probability,*Significant,**Non- significant.
In the present study, the infection rate of rotavirus was higher 20% than rate of other enteric viruses, this rate was comparable with result of study done by Mahmood et al21 in Baghdad (21%), Jaff et al.,22 in Sulaimani province with the (22%), and lower than that observed in Babylon (56%)23 and Erbil city (37%)24.
The percentages of adenovirus among diarrhea cases was18.75% and this percent was lower than Al-Khoweledy study in Al-Najaf province (23.33%), also this result agreement study of Mahmood et al21 rotavirus infections were higher than adenovirus in infants and young children in Baghdad, this may be related with similarity in studied area as well as transmission may occur via consumption of contaminated water, contaminated found or when people share personal objects.
Enteric viruses analysis showed that lower percent(13.75%) with norovirus and this result was lower than study of Ahmed26. Norovirus is the source in about 18% of all cases. Children and those in the developing world are most commonly affected27. Especially those below age five28. Also in the developing world children less than two years of age frequently get six or more infections a year29.
The present study also not recorded any positive astrovirus and this result disagreement with study done by Thewiny et al., in Basrah city, Who found prevalence of astrovirus was 2.6% among children under five years of age who were hospitalized with acute diarrhea in Basrah, Iraq. But astrovirus infection could be related to a mild diarrheal disease which would not require frequent hospitalization31,32
The present study showed that G. lamblia infection rate was (26.25%) this may be related with protozoan cysts are highly resistant to chlorine disinfection33.
This result comparable with study of Hussein [34] who found 23.7% in Thi-Qar province and higher than study of Salman et al.35 in Kirkuk province (9.35%). Recently, infection rate of G. lamblia was 9.5% in Duhok city and 5.7% in Erbil city [36], and 3.9% in Samarra37.
The result of current study has shown that high frequency associated with G. lamblia assemblage B (71.43%). This finding in agreement with other studies done in different places and had similar result such as38-43. This may be related with fact all patients with assemblage B show a greater rate of elimination of cysts. Also genotype A is also identified to most often responsible for the zoonotic spread with a broad range of animals offered as reservoir hosts, although assemblage B probably spread from human to human, it has been testified in some animals and may also be an animal potential44.
The differences in environmental and social condition might have contributed to the variations in the distribution of G. lamblia assemblages45. Therefore, the detection these factors may be lead to control on the parasitic infections.
According to co-infection with giardiasis, 14/42 cases had co-infection with rotavirus, 6/42 cases had co-infection with norovirus and 4/42 cases had co-infection with adenovirus and statistically significant. Co-infection can also increase treatment costs, probably as a result of clinical complications due to interactions among co-infecting pathogens.
Regarding age group most infection less than 5 years this causes could relate to the contaminated drinking water, and artificial milk in bottle, contaminated eating food or sucking pacifiers and personal hygiene measures, especially that age of creeping on ground as most parasites were belonging and they not realize the good sanitation in compare with other ages46.
Concerning the gender, this study revealed a high number of males patients than females patients which seem to be similar with study done by Mahmood et al (2015) in Baghdad, but statistically non-significant and this may be related with male and female were exposed to chance of infection due to all of them were living under the same conditions and climates of disease48.
In conclusion, infection rate of rotavirus amongst children in Diyala province appears to be relatively high than other enteric viruses. Co-infection with G. lamblia type B have important role in gastroenteritis. However, continued enteric virus surveillance and epidemiology amongst this group is required.
- Schlossberg D. Clinical infectious disease (Second ed.). 2015:p. 334. ISBN 9781107038912.
- Singh A. Pediatric Emergency Medicine Practice Acute Gastroenteritis. An Update. Pediatric Emergency Medicine Practice. 2010; 7(7):
- Ciccarelli S., Stolfi I, Caramia G. Management strategies in the treatment of neonatal and pediatric gastroenteritis. Infection and Drug Resistance. 2013;6: 133-61. 4- GBD. Mortality and Causes of Death, Collaborators. “Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015”. Lancet. 2015, 388 (10053): 1459-1544.
- Webber R. Communicable disease epidemiology and control : a global perspective (3rd ed.). Wallingford, Oxfordshire: Cabi. 2009: 79. ISBN 978-1-84593-504-7. Archived from the original on 2015-10-26.
- Eckardt AJ, Baumgart DC. Viral gastroenteritis in adults. Recent Patents on Anti-infective Drug Discovery. 2011; 6(1): 54-63. doi:10.2174/157489111794407877. PMID 21210762.
- Richard AH. Textbook of therapeutics: drug and disease management (8. ed.). Philadelphia, Pa.[u.a.]: Lippincott Williams and Wilkins. 2006: p. 2003. ISBN 9780781757348. Archived from the original on 2017-09-08.
- Szajewska H, Dziechciarz P. Gastrointestinal infections in the pediatric population. Current Opinion in Gastroenterology. 2010; 26(1): 36-44. doi:10.1097/MOG.0b013e328333d799. PMID 19887936.
- Meloni A, Locci D, Frau G, Masia G, Nurchi AM, Coppola RC. Epidemiology and prevention of rotavirus infection: an underestimated issue. Journal of Maternal-Fetal and Neonatal Medicine. 2011; 24(Suppl 2): 48-51. doi:10.3109/14767058.2011.601920. PMID 21749188.
- Webb A, Star, M. Acute gastroenteritis in children. Australian Family Physician. 2005; 34(4): 227-31. PMID 15861741.
- Adam RD, Eric WD, Craig AM, Daniel PB, Kent DB, Stacy MR, Matthew MH, Nirmala PN, Rima BP, Stephen FP, Theodore EN. Genome Sequencing of Giardia lamblia Genotypes A2 and B Isolates (DH and GS) and Comparative Analysis with the Genomes of Genotypes A1 and E (WB and Pig). Genome Biol Evol. 2013; 5(12): 2498–2511.
- Sahagún J, Clavel A, Goñi P, Seral C, Llorente MT, Castillo FJ, Capilla S, Arias A, Gómez-Lus R.Correlation between the presence of symptoms and the Giardia duodenalis genotype. Eur J Clin Microbiol Infect Dis. 2008; 27(1):81-3.
- Taherkhani H, Shariati S, Abdolahi N. Clinical manifestations of Giardiasis in Iran. Journal of clinical and diagnostic research. 2009; 3: 1416-1418.
- pelayo LA, Fraga J, Nunez FA, Mendoza, D, Torres DR, Finlay CM. Genetic characterization by random amplified polymorphic DNA analysis (RAPD) of 18 isolates of Giardia lamblia obtained from day care children. Exp Parasitol. 2003; 104(3-4): 162-6.
- Gelanew T, Lalle M, Hailu A, Pozio E, Cacciò SM. Molecular characterization of human isolates of Giardia duodenalis from Ethiopia. Acta Trop. 2007; 102(2):92-9.
- Helmy MM, Abdel-Fattah HS, Rashed L. Real-time PCR/RFLP assay to detect Giardia intestinalis genotypes in human isolates with diarrhea in Egypt. J Parasitol. 2009; 95:1000-1004.
- Koivunen, ME, Krogsrud RL. Principles of immunochemical techniques used in clinical laboratories. Lab. Med, 2006; 37: pp: 490-497.
- Sulaiman IM, Fayer R, Bern C, Gilman RH, Trout JM, Schantz PM, Das P, Lal AA, Xiao L Triosephosphate isomerase gene characterization and potential zoonotic transmission of Giardia duodenalis. Emerg Infect Dis. 2003; 14: 1444-52.
- Geurden T, Geldhof P, Levecke B, et al. Mixed Giardia duodenalis assemblage A and E infections in Alves. Int J Parasitol. 2007; 38(2008): 259-64.
- Geurden T, Levecke B, Cacció SM, Visser A, De Groote G, Casaert S, Vercruysse J, Claerebout E. Multilocus genotyping of Cryptosporidium and Giardia in non-outbreak related cases of diarrhea in human patients in Belgium. Parasitology. 2009; 136(10): 1161-8
- Mahmood DB, Raghad A, Faisal GA, Rafah AS. Detection of Adenovirus antigen and its correlation with clinical signs among children with gastroenteritis. Iraqi Journal of Science, 2015; 56(2): 1633-1638.
- Jaff DO, Tariq AG. Aziz, Natalie R. Smith. The Incidence of Rotavirus and Adenovirus Infections among Children with Diarrhea in Sulaimani Province, Iraq Journal of Biosciences and Medicines, 2016: 4: 124-131
- Al-Marzoqi AH, Shemmran, AR, Al-Nafee MK. Role of Rotavirus and Adenovirus in Acute Infantile Gastroenteritis in Infants Younger than One Year of Age in Babylon Province. Journal of Al-Qadisiyah for Pure Science. 2010; 15: 1-7.
- Ahmed, HM, Coulter JB, Nakagomi O et al. Molecular Characterization of Rotavirus Gastroenteritis Strains, Iraqi Kurdistan. Emerging Infectious Diseases. 2006; 12: 824-826. http://dx.doi.org/10.3201/eid1205.051422
- Al-Khoweledy Ahmed Jassim Shwalla. Detection of Adenovirus Type 40/41 Among Children With Diarrhea, In Al-Najaf province, Iraq. Journal of Babylon University – Pure and Applied Sciences. 2017; 25(3):
- Ahmed SM, Hall AJ, Robinson AE, Verhoef L, Premkumar PP, Umesh D; Koopmans M, Lopman, BA, Global prevalence of norovirus in cases of gastroenteritis: a systematic review and meta-analysis. The Lancet Infectious Diseases. 2014; 14(8): 725-30. doi:10.1016/S1473-3099(14)70767-4.
- Roger JW. Communicable disease epidemiology and control : a global perspective (3rd ed.). Wallingford, Oxfordshire: Cabi.2009: p.79. ISBN 978-1-84593-504-7. Archived from the original on 2015-10-26.
- Walker CL, Rudan I, Liu L, Nair H, Theodoratou E, Bhutta ZA, O’Brien KL, Campbell H, Black RE. Global burden of childhood pneumonia and diarrhoea. Lancet. 2013; 381(9875): 1405-16. doi:10.1016/S0140-6736(13)60222-6.
- Dolin R, Mandell GL, Bennett JE., eds. Chapter 93. Mandell, Douglas, and Bennett’s principles and practice of infectious diseases (7th ed.). Philadelphia, PA: Churchill Livingstone/Elsevier. 2010:ISBN 0-443-06839-9.
- Thewiny HT, Hassan JH, Basam DS. Human astrovirus among hospitalized children under five years of age with acute diarrhea in Basrah, Iraq. The Medical Journal of Basrah University, MJBU.2014, 32(2):70-76.
- Glass RI, Noel J, Mitchell D, Bresee JS, Stoll BJ. The changing epidemiology of astrovirus-associated gastroenteritis: a review. Arch Virol Suppl; 1996, 12: 287-300. 32-Medina S, Gutierrez MF, Liprandi F, Ludert JE. Identification and type distribution of astroviruses among children with gastroenteritis in Colombia and Venezuela. J Clin Microbiol 2000; 38: 3481- 3483.
- Graczyk TK; Shiff CK; Tamang L; Munsaka F; Beitin AM and Moss WJ. The association of Blastocystis hominis and Endolimax nana with diarrheal stools in Zambian school-age children. Parasitol Res. 2005; 98(1): 38.þ
- Hussein TK. prevalence and related risk factors for Giardia lamblia infection among children with acute diarrhea in Thi-Qar, southern Iraq. Thi-Qar Medical Journal. 2010; 4(4):2010:68-74.
- Salman YJ; Al-Taee ARA, Abid AM. Prevalence of Giardia lamblia among Iraqi displaced peoples in Kirkuk Province. Int J Curr Microbiol App Sci. 2016; 5(1): 753-760.
- Yilmaz H, Abdullah AM. Prevalence of Intestinal parasites (Entamoeba species and Giardia lamblia) in Duhok and Erbil cities, Northern Iraq. J Microbiol Exp 2017; 4(6): 00132.
- Bazzaz AA, Shakir OM, Alabbasy RH. Prevalence of two gastrointestinal parasites Entamoeba histolytica and Giardia lamblia within Samarra city, Iraq. Advances in Biosci and Biotechnol. 2017; 8(11): 399.
- Breathnach AS, McHugh TD, Butcher PD. Prevalence and clinical correlations of genetic subtypes of Giardia lamblia in an urban setting. Epidemiol Infect. 2010; 138(10):1459-1467.
- Al-Barghash MF. Molecular identification of Giardia duodenalis parasite isolate from human and animal by polymerase chain reaction – restriction fragment length Polymorphism technique (PCR-RFLP) in Baghdad province. MSc Thesis. College of Veterinary Medicine – University of Baghdad. 2009.
- Kohli A, Bushen OY, Pinkerton RC, Houpt E, Newman RD, Sears CL, Guerrant RL. Giardia duodenalis assemblage, clinical presentation and markers of intestinal inflammation in Brazilian children. Transactions of the Royal Soc. of Trop. Med. and Hygiene, 2008; 102(7): 718-725.
- Thompson RC, Monis P. Giardia-from genome to proteome. Adv Parasitol. 2012: 78(78): 57-95.
- Al-Difaie RS. Molecular Study to Detect Genotyping of Giardia lamblia from Human and Cattle Feces in Al-Qadisiya Governorate, Iraq. Ibn AL-Haitham J.Pure and Appl. Scie. 2017; 29(3): 1-13.
- Minetti C, Lamden K, Durband C, Cheesbrough J, Fox A, Wastling JM. Determination of Giardia duodenalis assemblages and multi-locus genotypes in patients with sporadic giardiasis from England. Parasites and Vect. 2015: 8(1): 444.
- Van Keulen H; Macechko PT, Wade S, Schaaf S, Wallis PM, Erlandsen SL. Presence of human Giardia in domestic, farm and wild animals, and environmental samples suggests a zoonotic potential for giardiasis. Vet Parasitol. 2002: 108(2): 97-107.
- Feng Y, Xiao L. Zoonotic potential and molecular epidemiology of Giardia species and giardiasis. Clin Microbial Rev. 2011: 24(1): 110-140.
- Al-Mamouri AK. Epidemiology of intestinal parasites and head lice in pupils of some primary school at Al-Mahaweel district, Babylon province. MSc. Thesis. Collge of Science. Babylon University. 2000: 122.
- Peterson KM. strategies for combating waterborne diarrheal disease in the developing world: investigating current appropriate technologies and communication methods in environmental public health. 2008.
© The Author(s) 2018. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.