


ISSN: 0973-7510
E-ISSN: 2581-690X
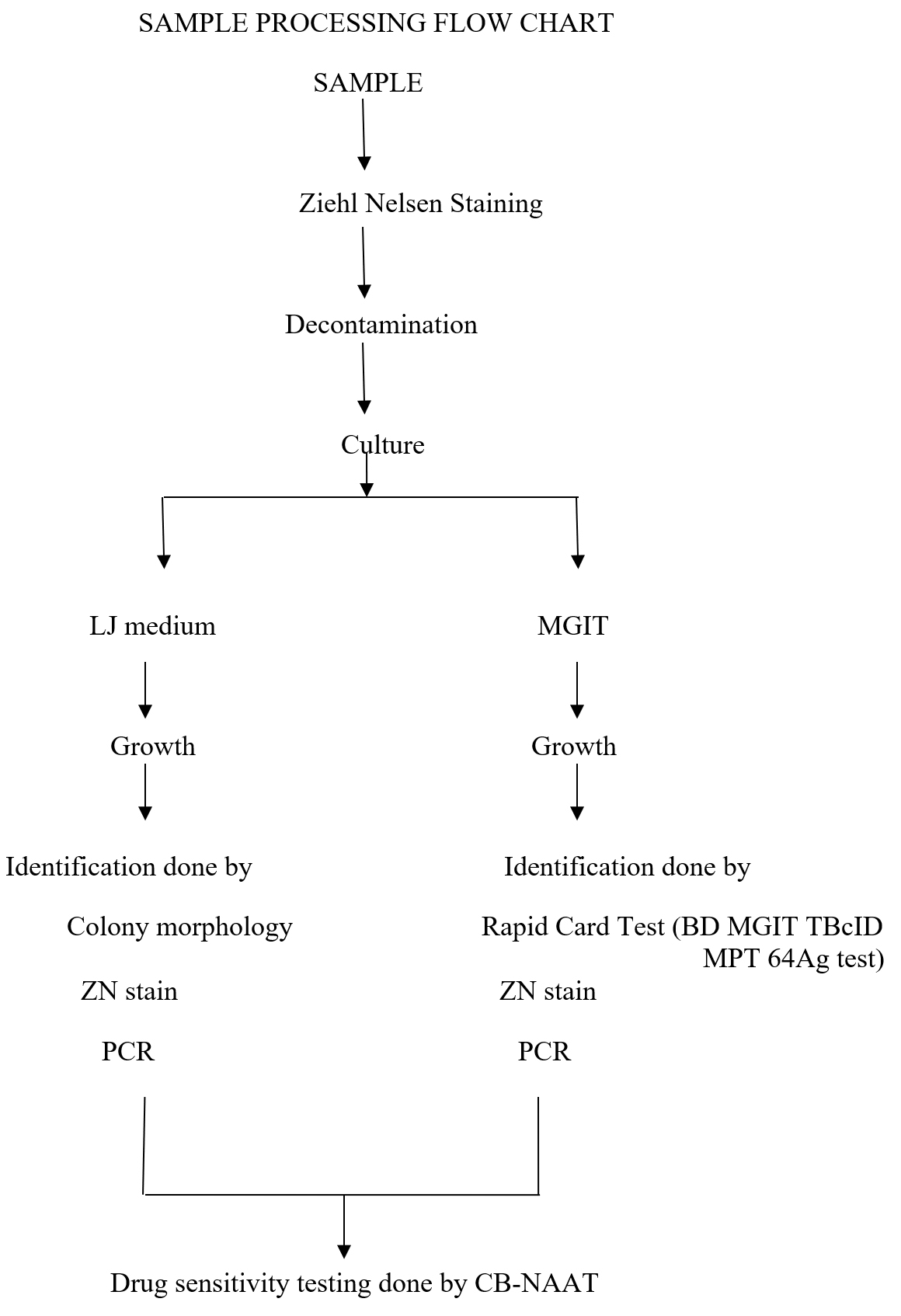
The objective of the present study is to find the prevalence of Mycobacterium tuberculosis from respiratory samples like sputum, BAL and pleural fluid, compare conventional LJ culture with rapid culture method i.e Mycobacterium growth indicator tube (MGIT) and to determine the pattern of drug resistance by automated methods i.e Gene Xpert. Respiratory samples were collected in sterile, wide-mouth, disposable, leak proof containers without any preservatives. Specimens were inoculated into MGIT for primary isolation of Mycobacteria. The specimen was processed according to the SOP manual provided by Becton Dickinson Company. The tubes were read for increasing fluorescence by MGIT reader. Reported results only when a MGIT tube was positive by the MGIT reader and smear made from the positive broth is also positive for AFB. For further identification, TBcID card test was put from MGIT positive tube and the result was given accordingly as mentioned in the procedure for TBcID kit insert. Polymerase chain reaction (PCR) was done in all 17 positive cases. The drug sensitivity test (CB-NAAT) was done at State Intermediate Reference Laboratory, Chandan Nagar, Dehradun, Uttrakhand as per RNTCP laboratory operational guidelines. In our study total number of samples received from the clinically suspected cases of pulmonary tuberculosis were 156, out of which 11% were positive and 89% were negative. The predominant age group involved was 51-60 years 24%, followed by 61-70 years 22%. In young children and adolescent age group very less number of samples were received i.e. 0-5%. Out of 17 positive samples, 94.11% (16/17) were detected as sensitive for Rifampicin and 5.89% (1/17) were resistant. On the statistical analysis of our data for MGIT, Positive Predictive Value (PPV) was 29% against Negative Predictive Value (NPV) of 100%. The specificity of MGIT was 92% against a sensitivity of 100%. Culture is still needed for species identification, confirmation and drug susceptibility testing. The diagnostic superiority of MGIT, both in terms of sensitivity and specificity has been proven better as compared to LJ in previous other studies and supported by our study as well. In our study, the diagnostic efficacy of MGIT culture was found to be superior as compared to the conventional LJ culture. The positivity rate was 10.89% (17/156) in MGIT & 3.2% (5/156) in LJ culture.
Rifampicin, LJ culture, PCR
Ancient history reveals that Tuberculosis (TB) has been one of the most primitive diseases of the mankind and has co-evolved with us since several million years ago. The causative agent Mycobacterium tuberculosis is an important human pathogen in virtually every part of the world1,2. Tuberculosis (TB) has a serious impact on global health and has recently become more problematic because of development of drug resistant strains in both developed and developing countries3. To effectively control tuberculosis is requirement in today’s world as it affects millions of people’s health across the world and hence needs to be put forward along with the basic principles of human right to health and social protection. TB epidemiology is closely connected with social and financial conditions of people. Since marginalized and vulnerable groups of people are greatly exposed to health problems, it makes the prevention, care and control of the disease even more challenging4.
Approximately 1.3 lakh new multi-drug resistant TB cases appear on a yearly basis in India which includes approximately 79,000 MDR-TB patients among notified pulmonary cases. India bears second highest number of estimated HIV associated Tuberculosis across the world. An estimated 1.1 lakh HIV associated TB occurred in 2015 and approximately 37,000 estimated number of patients died among them5. World Health Organization (WHO) in 2011 endorsed a novel, rapid and automated with molecular beacon technology to detect DNA sequences amplified in a hemi-nested real time PCR assay (Xpert MTB/RIF) that can simultaneously detect M. tuberculosis and rifampicin (RIF) resistance6.
The gold standard for diagnosis of tuberculosis till today is mycobacterial culture as it permits the diagnosis of drug resistance, including the emerging mutations. Traditional egg based (Lowenstein Jensen) and agar based (Middle brook 7H10/11) methods are widely used. The limit of detection is 100 bacilli/ml thus increasing the sensitivity compared to smear but the growth in a conventional egg-based medium takes four to eight weeks with an additional four weeks for drug sensitivity by the conventional proportion method. Thus, it takes a median of 70 days to diagnose a case of MDR-TB by conventional culture methods and the cultures require equipped and specialized labs and highly skilled staff7.
The most common detection method which has been endorsed by WHO in 2007 and adopted by RNTCP, is Mycobacterial growth indicator tube (MGIT), a liquid culture system, using Middle brook 7H9 broth a non radiometric detection method which measures the consumption of oxygen by fluorescence8. Xpert MTB/RIF (Cepheid) tests are expensive but marketed as point of care tests and require virtually no training and laboratory infrastructure. They are also designed for the rapid and simultaneous detection of M. tuberculosis and mutations associated with rifampicin resistance usually within 2 hours. This method has higher sensitivity i.e 95% and specificity 98% for tuberculosis detection in smear positive patient’s than in smear-negative patients in which sensitivity is 67% and specificity is 99%9.
A prospective study was conducted at the Department of Microbiology and Immunology, Shri Guru Ram Rai Institute of Medical & Health Sciences, Dehradun, Uttarakhand for a period of two years starting from March 2015 to February 2017. During this period 156 consecutive, non duplicate samples were collected. Samples were collected from suspected cases of tuberculosis, during the period of study from OPD and IPD services of various departments of SGRRIM & HS after obtaining written informed consent from patient. The period of study was two years; study was started after taking approval from Ethical Committee of SGRRIM&HS, Dehradun. Total 156 samples were collected during the study period.
Sample Collection and Transport10
Respiratory samples were collected in sterile, wide mouth, disposable, leak proof containers without any preservatives. Clinical details of patients were recorded. The samples were transported to laboratory as soon as possible after collection at 8˚C to inhibit the growth of unwanted micro organism and were processed within 48 hours of receiving in the laboratory.
(A) Inclusion criteria
Following respiratory specimens were included in our study:
- Sputum
- Bronchoalveolar lavage (BAL)
- Pleural fluid
(B) Exclusion criteria
- Samples less than 2ml.
- Pus
- Tissue
- Swabs
- CSF
- Salivary sample
- Samples preserved in formalin
Sample processing11-14
The Materials employed in present study were procured from Hi media Pvt. Ltd, Mumbai.
 *Routine biochemical tests and drug sensitivity testing was not performed due to cumbersome and time taking procedure
*Routine biochemical tests and drug sensitivity testing was not performed due to cumbersome and time taking procedure
Smears were prepared on a new, clean, unscratched glass slide over an area of 1 by 2 cm, heat fixed and stained by Ziehl Neelson stain. The smear was examined under oil immersion and reporting was done as per RNTCP guidelines.
Bronchoalveolar lavage and sputum sample were decontaminated by NALC-NaOH decontamination method as per standard protocol. Pleural fluid is a expected sterile fluid hence was processed directly for culture without decontamination. One slope per specimen was inoculated with a 5 mm loopful of the centrifuged sediment, distributed over the surface.
All cultures were incubated at 35-37°C until growth was observed or discarded as negative after eight weeks. Contaminated slopes were also discarded. AFB smears were prepared from positive MGIT culture tubes and result was given as follows.
- Smears were prepared, stained and looked for acid fast bacilli at 100x oil immersion.
- Sub culture was done on blood agar and incubated at 37°C for 48 hrs to confirm that there is no contamination.
- Reported results only when a MGIT tube was positive by the MGIT reader and smear made from the positive broth is also positive for AFB.
- For further identification BD MGIT TBcID card test was put from MGIT positive tube and result was given accordingly as mentioned in the procedure for TBcID kit insert.
Polymerase chain reaction (PCR) analysis (as per maufacturer’s instructions)
DNA extraction: (as per Qiagen DNA extraction kit instructions)
DNA Amplification: (as per manufacturer’s instructions, GeNei, Bangalore).
Target genes: IS6110
Interpretation
Positive result
Band at 123bp & (internal control band at 340bp).
Negative result
Band at 340bp (internal control) only.
Cepheid Xpert® MTB/RIF Assay15
All positive samples were subjected to CB-NAAT. The drug sensitivity testing (CB-NAAT) was done at state intermediate reference laboratory, Chandan Nagar, Dehradun, Uttrakhand as per RNTCP laboratory operational guidelines. The Guidelines for the specimen collection transport, handling and processing was followed as per the manufactures protocol.
Total number of samples received from the clinically suspected cases of Pulmonary and extra pulmonary tuberculosis were 156, out of which 17/156 (11%) came out to be positive. Number of negative cases were found to be 139 (89%).
Out of the total 156 samples were received from clinically suspected cases of pulmonary tuberculosis, maximum number received were of BAL 72% followed by pleural fluid 18% and sputum 10% (Table 1).
Table (1):
Sample wise distribution of suspected cases of tuberculosis (n=156 ).
| Types of sample | No. of cases (%) |
|---|---|
| Bronchoalveolar lavage | |
| (BAL) | 113(72%) |
| Pleural Fluid | 28(18%) |
| Sputum | 15(10%) |
Bronchoalveolar lavage (BAL) being the most predominant sample in our study, the positivity rate was 82%. Among the pleural fluid and sputum samples, positivity rate was 12% and 6% respectively (Table 2). As per Table 3 the predominant age group involved was 51-60 years 24%, followed by 61-70 years 22%. In young children and adolescent age group least samples were received i.e 0-5%.
Table (2):
Sample wise distribution of positive cases (n=17).
Types of sample |
Positive cases n=17 |
Percentage (%) |
|---|---|---|
BAL |
14 |
82 % |
Pleural Fluid |
2 |
12 % |
Sputum |
1 |
6 % |
Table (3):
Distribution of suspected cases according to age group (n=156).
| Age (in years) | Sample received (n=156) | Numbers of positive samples | |||
|---|---|---|---|---|---|
| Total No. |
Percentage (%) |
L J (n=5) |
MGIT (n=17) |
LJ & MGIT (n=5) |
|
| 0-10 | 0 | 0% | 0 | 0 (0%) | 0 |
| 11-20 | 8 | 5% | 0 | 0 (0%) | 0 |
| 21-30 | 17 | 11% | 0 | 2 (12%) p>0.01 | 0 |
| 31-40 | 17 | 11% | 1 | 1 (6%) p>0.01 | 1 |
| 41-50 | 18 | 11% | 0 | 3 (18%) p>0.01 | 0 |
| 51-60 | 37 | 24% | 1 | 2 (12%) p>0.01 | 1 |
| 61-70 | 34 | 22% | 3 | 6 (35%) p>0.01 | 3 |
| >70 | 25 | 16% | 0 | 3 (18%) p>0.01 | 0 |
Positivity of LJ culture and MGIT in various age groups was not found to be statistically significant (chi-square test, p value >0.01). In males the maximum numbers of positivity in MGIT culture was in age group 61-70 years 5 (42%), followed by age group more than 70 years 3 (25%), low positivity was seen in age group 31-50 years and 40-50 year 1 (1%) each. No positive case was observed in less than 30 years.
When comparing the findings with LJ culture, maximum positivity was shown in the same age group i.e. 61-70 years of age 2 (17%), followed by 51-60 yrs of age group 1 (8%). In rest of the age groups no positive cases were observed. In females, the maximum number of positivity in MGIT culture was shown in 21- 30 yrs & 61-70 yrs of age group 2 each (40%), followed by 41-50 yrs of age group 1(20%). No cases were observed in rest of the age groups & the difference in positivity according to age group was not found to be statistically significant (p value > 0.01).
When comparing findings with LJ culture, positivity was low only 1 case (20%), in age group 21-30 yrs & 61-70 year. In rest of the age groups no cases were observed & the difference in positivity according to age group was not found to be significant when checked on statistical basis (p value >0.01).
Amongst the positive cases males outnumbered females results were assessed by chi-square test and difference was not found to be significant when checked on statistical basis (p value>0.01). (Table 4 a & 4 b)
Table (4a):
Gender wise distribution of suspected cases (Male) (n=97).
| Age (in years) |
Male | Positive cases n=12 | ||
|---|---|---|---|---|
| Total No. of cases (n=97) |
Percentage (%) |
MGIT | LJ | |
| 0-10 | 0 | 0/97 (0%) | 0(0%) | 0(0%) |
| 11-20 | 5 | 5/97 (5%) | 0(0%) | 0(0%) |
| 21-30 | 9 | 9/97 (9%) | 0(0%) | 0(0%) |
| 31-40 | 13 | 13/97 (13%) | 1(8%) | 0(0%) |
| 41-50 | 10 | 10/97 (10%) | 1(8%) | 0(0%) |
| 51-60 | 22 | 22/97 (23%) | 2(17%) | 1(8%) |
| 61-70 | 19 | 19/97(20%) | 5(42%) | 2(17%) |
| >70 | 19 | 19/97(20%) | 3(25%) | 0(0%) |
Table (4b):
Gender wise distribution of cases (female) (n=59).
| Age (in years) |
Female | Positive Cases n=5 | ||
|---|---|---|---|---|
| Total No. of cases n=59 |
Percentage (%) |
MGIT | ||
| 0-10 | 0 | 0/59(0%) | 0/5 (0%) | 0(0%) |
| 11-20 | 3 | 3/59 (5%) | 0/5 (0%) | 0(0%) |
| 21-30 | 8 | 8/59(13%) | 2/5 (40%) | 1(20%) |
| 31-40 | 4 | 4/59 (7%) | 0/5 (0%) | 0(0%) |
| 41-50 | 8 | 8/59 (13%) | 1/5(20%) | 0(0%) |
| 51-60 | 15 | 15/59(25%) | 0/5 (0%) | 0(0%) |
| 61-70 | 15 | 15/59 (25%) | 2/5 (40%) | 1(20%) |
| >70 | 15 | 15/59 (25%) | 0/5 (0%) | 0(0%) |
Comparing ZN stain with MGIT culture, out of a total of 156 clinically diagnosed cases of pulmonary and extra pulmonary tuberculosis: 2 cases (1.28%) were positive in both ZN stain and LJ culture. 3 cases (1.92%) showed positivity in LJ culture and negative in ZN stain. 151 (96.79%) clinically suspected cases of tuberculosis were negative by both ZN smear and LJ culture.
The difference in positivity by both methods was found to be significant when checked on statistical basis (p value <0.01).
When comparing ZN stain with MGIT culture, Out of a total of 156 clinically diagnosed cases of pulmonary and extra pulmonary tuberculosis, 2 cases (1.28%) showed positivity in both ZN stain and MGIT culture. 15 cases (9.61%) showed positivity in MGIT culture and negative in ZN smear 139 (89.1%) suspected cases of pulmonary and extra tuberculosis were negative both by ZN smear and MGIT culture. The difference in positivity by both methods was found to be significant when checked on statistical basis (p value <0.01).
Time to detection of MGIT was as early as 19th day. Maximum positivity in MGIT was seen in 4th week of culture incubation. The mean time positivity was 23rd day (392/17). (Table 5 a) Time to detection in LJ was early as beginning of 5th week. 3 cases were detected positive in 6th week and one in 7th week. (Table 5 b)
Table (5a):
Time to detection (TTD) of culture positivity samples in MGIT.
| No. | Day of growth in weeks | |||||||
|---|---|---|---|---|---|---|---|---|
| 1st wk | 2nd wk | 3rd wk | 4th wk | 5th wk | 6th wk | 7th wk | 8th wk | |
| 1 | – | – | – | 23rd day | + | + | + | + |
| 2 | – | – | – | 28th day | + | + | + | + |
| 3 | – | – | – | 25th day | + | + | + | + |
| 4 | – | – | – | 28th day | + | + | + | + |
| 5 | – | – | – | 27th day | + | + | + | + |
| 6 | – | – | 20th day | + | + | + | + | + |
| 7 | – | – | 19th day | + | + | + | + | + |
| 8 | – | – | – | 24th day | + | + | + | + |
| 9 | – | – | – | 24th day | + | + | + | + |
| 10 | – | – | – | 23rd day | + | + | + | + |
| 11 | – | – | – | 25th day | + | + | + | + |
| 12 | – | – | – | 22nd day | + | + | + | + |
| 13 | – | – | – | 24th day | + | + | + | + |
| 14 | – | – | 20th day | + | + | + | + | + |
| 15 | – | – | 19th day | + | + | + | + | + |
| 16 | – | – | 20th day | + | + | + | + | + |
| 17 | – | – | 21st day | + | + | + | + | + |
Table (5b):
Time to detection (TTD) of culture positivity samples in LJ medium.
| No. | Growth in weeks | |||||||
|---|---|---|---|---|---|---|---|---|
| 1st wk | 2nd wk | 3rd wk | 4th wk | 5th wk | 6th wk | 7th wk | 8th wk | |
| 1 | – | – | – | – | – | – | 49th day | + |
| 2 | – | – | – | – | 38th day | + | + | + |
| 3 | – | – | – | – | – | 42nd day | + | + |
| 4 | – | – | – | – | – | 44th day | + | + |
| 5 | – | – | – | – | – | 43rd day | + | + |
Culture positivity in LJ was 5 out of 17 cultures positive in MGIT. 12 out of 17 MGIT positive samples were not grown in LJ media. Positive predictive value (PPV) was 29% against negative predictive value (NPV) of 100%. Specificity of MGIT was 92% against sensitivity of 100%.
Table (6):
Comparison of LJ and MGIT culture positivity (n=17).
| MGIT | L J culture | Total | |
|---|---|---|---|
| Positive | Negative | ||
| Positive | 5 | 12 | 17 |
| Negative | 0 | 139 | 139 |
| Total | 5 | 151 | 156 |
*Sensitivity 100%, Specificity 92%, PPV 29%, NPV 100%.
Table (7):
Contamination rate in MGIT and LJ culture.
Contamination rate |
Percentage % |
|---|---|
LJ |
8.2% |
MGIT |
9.4% |
The diagnostic efficacy of MGIT culture was found to be superior as compared with the conventional LJ culture. The contamination rate was 9.4% for liquid media (MGIT) and 8.2% for LJ medium. (Table 7). All the positive samples of MGIT were confirmed as positive by PCR. (Table 8) Out of 17 positive samples, 94% (16/17) were detected as sensitive for rifampicin and 6% (1/17) were found to be resistant. (Table 9)
Table (8):
MGIT culture positivity confirmation with PCR (n=17).
MGIT positive |
PCR confirmed |
|---|---|
17 |
17 |
Table (9):
Drugs sensitivity with CB-NAAT in Culture positive samples (n=17).
Name of Test |
Sensitive for Rifampicin |
Resistant for Rifampicin |
|---|---|---|
CB-NAAT |
16 |
|
(94.12%) |
1 (5.88%) |
The present study was planned to compare the Mycobacteria growth indicator tube (MGIT), a liquid media based culture method with the conventional solid culture i.e. LJ for recovery of Mycobacterium tuberculosis.
Considering samples from suspected cases, majority of them were of BAL (72%), followed by pleural fluid 28 (18%) and sputum 15 (10%). In another study from India Rodrigues et al in 2009, reported majority of samples were of sputum (62%) followed by BAL (36%)16. In 2016 a study from North East India, Bhattacharya et al reported pleural effusion (30.04%) was the commonest sample amongst extra pulmonary tuberculosis17.
Predominant age group involved in our study was 51-60 yrs (24%) followed by 61-70 yrs (22%), & least age group involved was 11-20 yrs (5%). No samples were received from <10 yrs of age group. Ravi Kumar et al from Karnataka in 2018 has reported 29.1% were in the age group 30-44 years, followed by 27% in the age group of 45-59 years which is similar to our study18. Contrary to our study Tudu et al from Jharkhand in 2017, reported higher number of cases in younger age group of 15-25 (27.7%), followed by 26-35 years age group (27.3%) and 36-45 yrs age group (21.7%) and least were in age group of more than 65 yrs (3.3%)19.
In our study, males out number (62.17%) as compared to females (37.82%) which is similar to other studies like reported by Tudu et al from Jharkhand in 2017, male (70%) vs. female (30%), Jimenez Coron, et al. in 2009 (58%) males vs. female (41.1%), Ratnesh et al from UP as male (55.9% ) vs. Female (44.1%)19-21.
2 cases out of 156 (1.28%) suspected cases showed positivity in both ZN stain and LJ culture whereas 3 (1.92%) showed positivity only in LJ culture. Bhat et al from Mangaluru in 2018, showed that 20 cases out of 100 (20%) suspected cases were positive in both ZN stain and LJ culture, which is quite high as compared to our finding22.
When comparing ZN smear with MGIT culture, Out of a total of 156 clinically diagnosed cases of pulmonary & extrapulmonary tuberculosis, 2 cases (1.28%) showed positivity in both ZN stain and MGIT culture. Bhat et al from Mangaluru in 2018, showed that 21 cases out of 100 (21%) suspected cases were positive in both ZN stain and MGIT culture, which is quite high as compared to our finding. 15 cases (9.61%) in our study showed positivity only in MGIT culture but negative in ZN stain, where as Bhat et al reported only 2 cases which were negative in ZN stain but positive in MGIT culture, which is quite low as compared to our finding22.
In our study smear positive samples were 2 (1.28%), which came out to be positive in both LJ media as well as in MGIT. Getu Diriba et al from Ethiopia in 2017 reported the recovery rate for LJ and MGIT, for smear positive samples was 66.7% (74/111) and 87.4% (97/111) respectively while for smear negative samples was 13.4% (108/797) and 17.4% (139/797) for LJ and MGIT methods respectively23.
Our study compared MGIT with established conventional culture technique (LJ) for Mycobacterium tuberculosis and focused upon two important variables in a media i.e the rate of retrievel and mean time to detection i.e. sensitivity and speed. The possibility of inclusion of bias in such type of comparative studies can not be ignored which nevertheless can be eliminated if we follow standardized protocol. First the reading frequency was not the same for the two types of media, for MGIT reading was daily for the first 3 weeks and twice weekly thereafter, for solid media reading was once weekly and secondly the contamination rate of the two culture media. In our study the contamination was not very high, for liquid media (MGIT) was 9.4% and for LJ it was 8.2% and parallels the findings of Palaci et al24, whereas Rishi et al. has mentioned 13.7% contamination rate in MGIT and 27.2% in LJ. Chihota et al. have mentioned 16.7% contamination in MGIT and 9.3% in LJ.25,26.
In our study the total number of samples received from the clinically suspected cases of Pulmonary & extra pulmonary tuberculosis were 156. The positivity rate was 10.89% (17/156) in MGIT & 3.2% (5/156) in LJ which is comparable with the study done by Fadzilah et al (11.8%) in MGIT& 6.1% in LJ in 2009 in Malaysia27. Rishi et al. from Jaipur in 2007, reported the positivity rate for both pulmonary as well as extra pulmonary samples for M960 system as 34.10% (88/258) and of LJ as 1.93% (5/258) which is quite high for MGIT but comparable with LJ.25 Chihota et al. in 2010 from UK reported a higher positivity rate as compared to our study for both MGIT as well as LJ as 29.7% & 22.8% respectively26.
In our study, out of total 156 samples received in LJ culture there were total 5 (3%) cases which were positive. when comparing with MGIT culture there were total 17 cases which were positive (11%). Chien et al. from Taiwan in 2000 reported BACTEC MGIT 960 positivity rate as 32% & that of LJ as 25.8%28. Otu et al. from Gambia in 2008 reported BACTEC MGIT 960 detected 57.1% and LJ medium detected 43.5% specimens with Mycobacterium tuberculosis complex29. Bhat et al. from Mangaluru in 2018, showed 23% positivity in MGIT culture which is comparable to our study & 21% positivity in LJ which is quite high as compared to our study22.
The above findings also indicate better diagnostic efficacy of MGIT vs. LJ culture technique. In our study the mean time for detection of growth in MGIT was 23 day which earlier than that on LJ medium (43.2 day). Palaci et al.24 reported the mean time for the detection of growth in MGIT as 12.5 day which was also one week earlier than that on LJ medium (19.5 day). Rishi et al.25 has reported the mean time for the detection of growth in MGIT as 9.66 days and that of LJ as 28.81 days which is approximately 3 weeks earlier than that on LJ medium.
The above findings have reported the positivity of MGIT earlier as compared to our study. The reason may lie in the volume of specimen which we are using for sample processing. Due to various reasons sometimes the volume of specimen which reaches to the laboratory is around 2ml, which becomes a major constraint in getting positive earlier.
In our study when testing for drug sensitivity by Cartridge based nucleic acid amplification technique (Gene Xpert), out of 17 positive samples, 94% (16/17) were detected as sensitive for rifampicin (RIF) and 6% (3/17) were found to be RIF resistant TB. Shetye et al. from Mumbai, in their study have reported 28% RIF positive rate (resistant) higher as compared to our study30. Guenaoui K has reported upto 42% RIF resistance in suspected multidrug resistant pulmonary tuberculosis cases Algeria in 201631.
ACKNOWLEDGMENTS
We acknowledge the support of Dr Narottam Sharma, incharge molecular laboratory SGRRIMHS for providing assistance in molecular work. We would like to thank State TB reference laboratory Chandan Nagar Dehradun for providing assistance in data management of patients related to drug sensitivity testing.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
VK, NN designed the manuscript, BCP performed the experiments and gathered the information from literature, VK, NN, DR, IC, HS analysed the data, VK, NN, DR, IC, HS drafted the manuscript, VK supervised the manuscript, NN reviewed the manuscript and designed the tables.
FUNDING
None.
ETHICS STATEMENT
This study was carried out after taking approval from Ethical committee of Sri Guru Ram Rai Institute of Medical and Health Sciences Patel Nagar Dehradun.
AVAILABILITY OF DATA
All data sets generated or analysed during the study are included in the manuscript .
- Hirsh AE, Tsolaki AG, DeRiemer K, Feldman MW, Small PM. Stable association between strains of Mycobacterium tuberculosis and their human host populations. Proc Natl Acad Sci USA. 2004;101(14):4871-4876.
Crossref - Daniel TM. Captain of death: the story of tuberculosis. Rochester (NY): University of Rochester Press. 1997.
- Park YK, Park YS, Na KI, Cho EH, Shin SS, Kim HJ. Increased tuberculosis burden due to demographic transition in Korea from 2001 to 2010. Tuberc Respir Dis. 2013;74(3):104-110.
Crossref - Lacerda SNB, De Abreu Temoteo RC, de Figueiredo TMRM, et al. Individual and social vulnerabilities upon acquiring tuberculosis: a literature systematic review. Int Arch Med. 2014;7:35.
Crossref - Revised National TB Control Programme. TB India 2017. Annual Status Report. Ministry of health and family welfare, Central TB Division, Directorate General of Health Services. New Delhi: RNTCP: 2017. http://www.tbcindia.gov.in
- World Health Organization. Automated real-time nucleic acid amplification technology for rapid and simultaneous detection of tuberculosis and rifampicin resistance: Policy statement: Xpert MTB/RIF system. Geneva: WHO, 2011. http://www.who.int/iris/handle/10665/44586#sthash.Cdd-BEYMy.dpuf.
- Shah NS, Moodley P, Babaria P, et al. Rapid diagnosis of tuberculosis and multidrug resistance by the microscopic-observation drug-susceptibility assay. Am J Respir Crit Care Med. 2011;183(10):1427-1433.
Crossref - World Health Organization. New Laboratory Diagnostic Tools for Tuberculosis Control. Geneva: WHO, 2008. http://www.stoptb.org/assets/documents/global/retooling/Diagnostic_Brochure_Print_200 9_Jan_29.pdf.
- Steingart KR, Schiller I, Horne DJ, Pai M, Boehme CC, Dendukuri N. Xpert MTB/RIF assay for pulmonary tuberculosis and rifampicin resistance in adults. Cochrane Database Syst Rev. 2014;2014(1):CD009593.
Crossref - Monika Cheesebrough. Microbiological tests. Distric Laboratory Practice in Tropical Countries: 2nd ed. New York: Cambridge University Press. 2007:6-9.
- Revised National TB Control Programme. Standard Operative Procedure for collection, transport and processing and inoculation of extra-pulmonary specimens. Ministry of health and family welfare, Central TB Division, Directorate General of Health Services. New Delhi. RNTCP. 2016. http:// www. tbcindia. nic. In / index1.php?lang=1&level=2&sublinked=4573&lid=3177.
- Chatterjee M, Bhattacharya S, Karak K, Dastidar SG. Effects of different methods of decontamination for successful cultivation of Mycobacterium tuberculosis. Indian J Med Res. 2013;138(4):541-548.
- Winn WC, Koneman EW, Allen SD, et al. Mycobacteria. In: Joyce J, Larkim J, editors. Koneman’s color Atlas and Textbook of Diagnostic Microbiology: 7th ed. China: Lippincott williams and willkins. 2006:22-25.
- Nolte FS, Metchock B. Mycobacterium. In: Murray PR, Baron EJ, Tenover FC, Yolken RH, editors. Manual of Clinical Microbiology: 6th ed. Washington DC. American Society for Microbiology. 1995:351-52.
- World health organization. Xpert MTB/RIF system for the diagnosis of pulmonary and extrapulmonary TB and rifampicin resistance in adults and children. Geneva: WHO. 2013. http://www.stoptb.org/wg/gli/assets/documents/WHO Policy Statement on Xpert MTB-RIF 2013 pre publication 22102013.pdf. 134
- Rodrigues C, Shenai S, Sadani M, et al. Evaluation of the bactec MGIT 960 TB system for recovery and identification of Mycobacterium tuberculosis complex in a high through put tertiary care centre. Indian J Med Microbiol. 2009;27(3):217-221.
Crossref - Bhattacharya PK, Jamil MD, Lyngdoh M, Akhtar H, Roy A, Talkadar KK. Spectrum of pulmonary and extra pulmonary Tuberculosis: A retrospective study from Northest India. National Journal of Laboratory Medicine. 2016;5(4):1006-1010.
- Ravikumar P, Priyadarshini BG. A study of extra-pulmonary tuberculosis and its outcome. Int J Adv Med. 2017;4(1):209-213.
Crossref - Tudu L, Munda VS, Haider S, Kashyap V. A Study on Socio Demographic Profile of Pulmonary Tuberculosis Patients Attending Dots Centre of Field Practice Area of Rajendra Institue of Medical Sciences, Jharkhand. IOSR-Journal of Dental and Medical Sciences. 2017;16(6):126-130.
Crossref - Jimenez-Coron, M, Garcia-Garcia L, DeRiemer K, et al. Gender differentials of pulmonary tuberculosis transmission and reactivation in an endemic area. Thorax. 2006;61(4):348-353.
Crossref - Ratnesh, Singh AK, Gupta SB. Socio demographic profile of tuberculosis patients under RNTCP in district Bareilly. Indian Journal of Forensic and Community Medicine. 2017;4(1):46-48.
Crossref - Bhat UP, Boloor R. Comparison of Rate of Isolation and Characterisation of Mycobacteria by AFB Smear, LJ Medium and MGIT. Int J Curr Microbiol App Sci. 2018;7(1):2397-2404.
Crossref - Diriba G, Kebede A, Yaregal Z, et al. Performance of Mycobacterium Growth Indicator Tube BACTEC 960 with Lowenstein-Jensen method for diagnosis of Mycobacterium tuberculosis at Ethiopian National Tuberculosis Reference Laboratory, Addis Ababa, Ethiopia. BMC Research Notes. 2017;10(1):181.
Crossref - Palaci M, Ueki SYM, Sato DN, Curcio M, Silva EAM. Evaluation of Mycobacteria Growth Indicator Tube for recovery and drug susceptibility testing of Mycobacterium tuberculosis isolates from respiratory specimens. J Clin Microbiol. 1996;34(3):762-764.
Crossref - Rishi S, Sinha P, Malhotra B, Pal N. A comparative study for the detection of Mycobacteria by BACTEC MGIT 960, Lowenstein Jensen media and direct AFB smear examination. Indian J Med Microbiol. 2007;25(4):383-386.
Crossref - Chihota VN, Grant AD, Fielding K, et al. Liquid vs. solid culture for tuberculosis: performance and cost in a resource-constrained setting. Int J Tuberc Lung Dis. 2010;14(8):1024-1031.
- Fadzilah N, Ng KP, Ngeow YF. The manual MGIT system for the detection of M. tuberculosis in respiratory specimens: An experience in the University Malaya Medical Centre. The Malaysian Journal of Pathology. 2009;31(2):93-97.
- Chien HP, Yu MC, Wu MH, Lin TP, Luh KT. Comparison of the BACTEC MGIT 960 with Lowenstein-Jensen medium for recovery of Mycobacterium from clinical specimens. Int J Tuberc Lung Dis. 2000;4(9):866-870.
- Out J, Antonio M, Cheung YB, et al. Comparative evaluation of BACTEC MGIT 960 with BACTEC 9000 MB and LJ for isolation of mycobacteria in the Gambia. J Infect Developing Countries. 2008;2(3):200-205.
Crossref - Shetye S, Chheda P, Lad A, Matkar S.Performance of Xpert MTB/RIF assay for detection of M.TB in pulmonary and extra pulmonary samples in Indian patients. SAARC J Tuber Lung Dis Hiv/Aids. 2017;14(1):7-12.
Crossref - Guenaoui K, Harir N, Ouardi A, et al. Use of GeneXpert Mycobacterium tuberculosis/rifampicin for rapid detection of rifampicin resistant Mycobacterium tuberculosis strains of clinically suspected multi-drug resistance tuberculosis cases. Ann Transl Med. 2016;4(9):168.
Crossref
© The Author(s) 2021. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.