


ISSN: 0973-7510
E-ISSN: 2581-690X
Essraa A. Hegazy1 and Lamiaa A. Madkour1
This study was carried out in the dental school of Ahram Canadian University in Egypt to investigate the knowledge and compliance of senior students and interns toward infection control practices. A self‑administered questionnaire was employed with questions pertinent to the participants’ knowledge of risks in the dental settings, the practice of hand hygiene, the use of protective equipment, and the management of sharp injuries, among others. Although the knowledge and practice of the 240 surveyed participants were good; they were not up to the coveted standards. Despite being an integral part of their curriculum, an alarming percentage (19.6%) of the participants denied receiving knowledge about infection control instructions. Meanwhile, only 72.5% were aware of being at risk in the dental settings, and 78.3% confirmed their practice of hand hygiene. On the other hand, 84.6% of the surveyed participants confirmed the availability of protective equipment and 94.2% of them expressed their willingness to apply infection control measures in the future. The defects in the knowledge and practice mandate corrective actions to promote and upgrade the students’ compliance. Meanwhile, other gaps can be rectified via developing state-of-the-art communicative strategies. Efforts are warranted to enhance the attitude and motivate the students to conform to the protective safety measures. With all the infection control procedures already established in dental schools, the challenge lies in improving the students’ compliance with these recommendations.
Dental clinics, Hand hygiene, HBV, Infection control, PPE, Sharp injuries
Dental health practitioners (DHP) are at high risk of exposure to blood-borne pathogens, such as hepatitis B virus (HBV), hepatitis C virus (HCV), and human immunodeficiency virus (HIV) through contact with patient’s blood and fluids. Other risks include exposure to airborne microbes and injuries with contaminated sharp instruments.1-3 With an escalation in the prevalence of infectious diseases among dental patients, infection control practices are gaining a wider spotlight as pivotal elements in clinical dentistry.4 Health-care personnel in all settings are expected to know and practice the standard precautions which are essentially designed to protect them against acquiring infections, as well as to halt the spread of infection among patients.4,5
In the meantime, a higher concern is required during dental endeavors such as preparation of medications, administration of local anesthesia, as well as sterilization of dental cartridges and syringes between patients. Limited application of infection prevention guidelines in dental practice eventually leads to cross-infection. Unsafe practices such as the 1) use of a single syringe to administer medication to multiple patients, 2) re-insertion of a used syringe into a medication vial or solution container for the same patient or subsequent patients, 3) preparation of medications in proximity to contaminated supplies or equipment and 4) inappropriate sterilization of needles and cartridges containing local anesthesia between patients lead to inevitable transmission of infection within the clinical environment.5,6
Implementing the recommended infection control procedures in dental schools and clinics is fundamental. Awareness and compliance with these recommendations are crucial for the prevention of nosocomial and occupational infections among the DHP.7 Unfortunately, implementation of infection control measures is limited to a few DHP in their clinical practice.8 This necessitates a high level of medical training, clinical skills, as well as knowledge for the undergraduate students so that they can adopt appropriate attitudes and behaviors in infection control when they become professionals.9,10 Throughout this study, we aimed to assess the awareness, knowledge, attitude, and practice among undergraduate dental students and interns toward infection control measures in dental clinics. The purpose was to determine to what extent the dental students are evaluating the risk of infectious diseases and protecting themselves and their patients.
Ethical Consideration
Institutional ethical clearance for the approval of this study was obtained. Approval of the study design and steps was conducted with the Head of the Infection Control Committee in Ahram Canadian University (ACU). Dental students and interns participated voluntarily and informed consent was obtained after explaining the nature of the study to all participants.
Study design
A cross-sectional descriptive survey was adopted to assess compliance with the infection control measures in dental clinics.
Target population
Fourth-, fifth-grade dental students and interns who attended the infection control course and the clinical training in the form of lectures and on-job training were invited to participate in the study. Students who have postponed the course were excluded.
Study setting
The Hospital of ACU with its educational and private dental clinics represented a well-equipped environment to carry out the survey. The researchers collected information by interacting with participants.
Data collection methods and tools
Employing Microsoft Excel, the data were organized and analyzed. A total of 240 out of 813 dental students agreed to fill out and complete the questionnaire without discussing it with their friends. The questionnaire was completed in no more than 10 minutes. A self-administrated anonymous and confidential English-language questionnaire consisting of 31 close-ended questions aimed to A) Assess the knowledge and attitude of students regarding adherence to hand hygiene, personal protective equipment (PPE), willingness to treat patients with infectious diseases and following infection control guidelines in the future, B) Evaluate the knowledge related to percutaneous and mucous membrane exposure, HBV vaccination, availability and selection of PPE, availability of supplies for different types of hand hygiene, respiratory hygiene, sterilization, and environmental decontamination, care of dental unit waterlines, safe injection practices, and proper sharps disposal.
To assure the ease of reading, clarity of wording, and understanding of the questions, the questionnaire was administered to 20 students in a pilot study, and a few modifications were introduced. The students enrolled in the pilot study were excluded from the final sample. The survey questionnaire was prepared based on the CDC guidelines.5
Statistical Analysis
Data from all returned questionnaires were entered and analyzed using SPSS 21.0 (IBM Corporation, Armonk, NY, USA). Frequencies and percentages were calculated. For assessment of associations between variables, the Chi-squared test was employed. The level of statistical significance was set to P < 0.05.
A total of 240 study participants were interviewed with self-administered questions to assess their knowledge and compliance towards the measures of infection control. The participants had an age range from 21-27 years old with a mean age of 22.73, and 50.4% of them were females.
The participants included 59 interns, 90 4th-grade students, and 91 5th-grade students, representing 24.6%, 37.5%, 37.9% of the study sample respectively. The majority of the respondents (75%) were undergraduate students.
The questionnaire required data on knowledge, attitude, as well as the practice of infection control procedures, orientation about occupational risk in dental procedures, immunization against HBV, hand hygiene, sterilization, wearing of gloves, masks, eye shields, the use of disinfectants after every patient, blood spillage management, environmental cleaning, and monitoring of infection control strategy.
The primary dependent variable was passing the infection control course during the college study duration, where all participants approved receiving and passing the course exam.
Upon inquiring about receiving any infection control application instructions during training, 193 participants (80.4%) declared their receipt of infection control instructions, while 47 (19.6%) denied receiving them (Fig. 1).
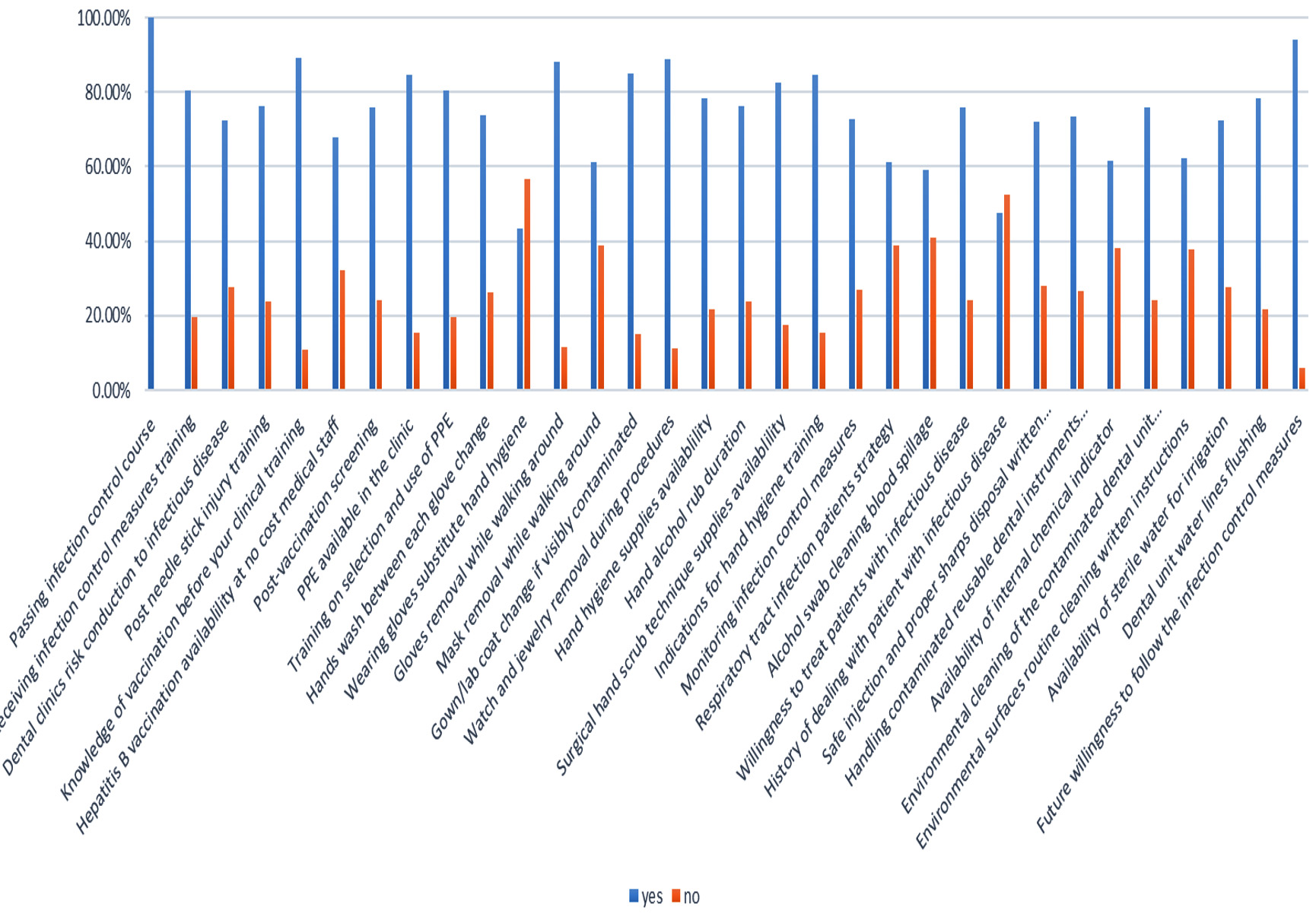
Fig. 1. Participants’ responses to the survey questions.
On interrogating them about infectious disease transmission risk in dental clinics, 174 participants (72.5%) claimed their awareness of being at risk, while 66 (27.5%) denied being at risk (P-value= 0.010).
Out of 240 participants, 183 (76.3%) were knowledgeable about post-needle stick injury management, 214 (89.2%) knew the vaccination list they had to receive before clinical practice, where 163 (67.9%) of them stated their knowledge about HBV vaccination availability at no cost to medical personnel (P-value= 0.005) and 75.8% of the participants underwent post-vaccination screening to detect protective anti-viral antibodies.
Regarding PPE, about 203 participants (84.6%) admitted the availability of PPEs in dental clinics including examination gloves, surgical face masks, protective clothing, protective eyewear/face shields, utility gloves, and sterile surgeons’ gloves for surgical procedures (P-value= 0.002) Meanwhile, 193 participants (80.4%) had confirmed receiving training on proper selection and use of PPEs.
On analyzing the way they deal with masks and gloves in between patients, and when they change their lab coat, 147 participants (61.3%) declared removing the mask and 212 (88.3%) declared gloves removal while walking around, while 204 (85.0%) stated changing their gown/lab coat if visibly contaminated.
Upon asking about hand hygiene practices, 188 participants (78.3%) confirmed their practice of hand hygiene; where 213 (88.8%) removed their watches and jewelry during any procedure and 177 (73.8%) recorded washing their hands between each glove change. However, 104 participants (43.3%) thought that wearing gloves is a good substitute for hand hygiene and they don’t have to wash hands after gloves removal.
Upon probing them about alcohol-based hand rub, 203 participants (84.6%) were recorded to be trained regarding appropriate indications for hand hygiene, including handwashing, hand antisepsis, and surgical hand antisepsis. Meanwhile, 198 participants (82.5%) confirmed the availability of supplies for surgical hand scrub technique (P-value = 0.015) and 183 (76.3%) of them knew the proper duration for alcohol rub, which is 20 seconds.
Upon inquiring about being monitored regarding infection control practices such as immunizations, hand hygiene, and sterilization, about 175 participants (72.9%) declared having a monitoring system for infection control practices, and 148 (61.7%) confirmed the availability of sterilization monitoring system using the internal chemical indicator in each sterilized dental instrument pouch (P-value= 0.008)
On probing about respiratory tract infected patients protocol and the way of dealing, 147 participants (61.1%) stated that the clinic offers instructions at entrances to patients with symptoms of respiratory infection and the way of dealing with their secretions, while 93 participants (38.9%) denied their knowledge.
On asking about the management of oral blood spillage, safe injection, and proper sharps disposal orientation, 142 participants (59.2%) were recorded to clean patient blood spillage with an alcohol swab, while 173 (72.1%) stated the availability of written recommendations regarding safe injection and proper sharps disposal at clinics, and 176 participants (73.3%) confirmed the availability of instructions for handling contaminated reusable dental instruments at the clinic (P-value= 0.016).
Upon asking them about their intention and willingness to treat patients with infectious disease, 182 participants (75.8%) revealed their intention to deal with them and 114 (47.5%) participants stated that they had already dealt with them in the past.
Regarding environmental cleaning instructions, 182 participants (75.8%) approved the presence of strategy for dealing with contaminated dental units after treating patients (P-value= 0.042), where 149 (62.1%) confirmed the presence of written instructions available for routine cleaning and disinfection of environmental surfaces (P-value= 0.051).
Regarding water system infection control measures, 174 participants (72.5%) asserted the availability of sterile water used for irrigation and 188 (78.3%) (P-value= 0.031) confirmed the routine flushing of the dental unit water lines at the start of the day for 2 minutes and in between patients for 20-30 seconds.
Upon questioning the surveyed participants about their willingness to follow the infection control measures that they were trained on in the future, 226 of them (94.2%) confirmed their willingness, while 14 (5.8%) showed their disinterest in applying those measures in their upcoming future work.
The awareness and practice of infection control measures have been proven to be indispensable for DHP. With the ever-changing worldwide circumstances, regular re-evaluation of this awareness has become a pressing need.
The participants enrolled in this study attend infection control lectures throughout the first year of the undergraduate program. Practice guidelines are part of their fourth-year clinical training. A standard infection control protocol is adopted at the ACU, and the faculty pays due attention to students’ adherence to the recommended infection control measures.
Despite these facts, an alarming percent (19.6%) of the enrolled subjects denied receiving knowledge about infection control instructions. This might reflect either the reluctance of these students to attend courses in general, or their view of infection control courses, in particular, as subsidiary or even unnecessary.
In assessing the participants’ knowledge, 72.5% of them admitted they were aware of being at risk in the setting of the dental clinics. This was somewhat close to the percentage of 67% reported by El-saaidi et al.11 Nonetheless, a lower percentage of 60.2% was reported by Ravichandran et al.12 And in contrast, a higher percentage of 84.8% was reported by Assiri et al.13 Meanwhile, 76.3% of the participants were knowledgeable about post-needle stick injury management. Other studies from Morocco and India showed remarkably low percentages of 50% and 32.2% respectively.14,12
Given (1) the frequent use of sharp instruments in dental clinics and the subsequent possibility of the spread of blood-borne viruses (2) and the high risk of inhalational transmission, insufficient knowledge about such risks should be taken seriously. This knowledge defect can be amended via tailored awareness programs that comprise regular sessions and training workshops for all undergraduate students. Additionally, refreshing the students’ knowledge just before their graduation can augment the impact of these programs.
Among the enrolled participants, 89.2% knew the vaccination list they had to receive; however, only 67.9% of them knew that HBV vaccination is available at no cost to medical personnel. In the meantime, 75.8% of the participants underwent post-vaccination screening to detect protective antibody levels. This was quite close to the percentage of 75.9% reported by Assiri et al.13; however, a much lower percentage of 13.9% was reported by Ravichandran et al.12 The lack of knowledge about vaccine availability and post-vaccination screening implies a communication gap between the organizations offering the vaccines and their target populations. This gap has to be addressed through modern communication technologies that spread on a wider base and readily reach all those concerned.
Of the 240 participants, 84.6% admitted the availability of PPEs, and 80.4% confirmed receiving training on their use. This percentage was in line with another study from Egypt, where 85.8% of the students were aware of donning PPEs during procedures.15 On the other hand, a study from India showed that only 68.9% of students knew about the proper use of PPEs.12
Personal protective equipment, including gowns, goggles, masks, and gloves has proven to be effective means of preventing pathogen transmission.16 Although our result was relatively higher than other studies; yet, any failure to comply with the proper use of PPEs can harm not only the patients but also the healthcare teams. Hence, regular inspection in dental settings is justifiable to ensure conformance to wearing the PPE.
Out of the surveyed subjects, 78.3% confirmed their practice of hand hygiene and 88.8% removed their watches and jewelry during any procedure. In addition, 73.8% recorded washing their hands between each glove change, while 43.3% thought that they don’t have to wash their hands after gloves removal.
In concordance with these results, Ravichandran et al.12 demonstrated that 79.2% of their participants regularly washed their hands. However, a higher percentage of 93.6% was obtained by Qamar et al.17 On the other hand, Hbibi et al.14 and Halboub et al.7 demonstrated that participants who regularly adhered to handwashing were only 47% and 43% respectively. In the same context, Assiri et al. demonstrated that 61.5% of participants removed their accessories during dental procedures,13 while Halboub et al.7 demonstrated that 44.9% of participants removed their jewelry and watches during procedures. In light of the worldwide pandemics, such discrepant percentages dictate not only the continuation and reinforcement of the current education and training about hand hygiene but also the encouragement of students to attend and commit to such training as part of an obligatory course.
Concerning PPE removal while walking around, 61.3% of the subjects declared removing the masks and 88.3% declared gloves removal, while 85% declared changing their gown/lab coat if visibly contaminated. Variable percentages were revealed from different countries. A study from Yemen revealed that 53.1% of the participants removed gloves and masks while moving around, and 87.5% changed their lab coats if soiled.7 A study from Morocco revealed that 72.3% of participants changed their gown/coat when soiled.14 Meanwhile, higher rates were revealed in a study from Saudi Arabia where 94.9% of participants removed masks and gloves while walking around, and 97.4% changed their lab coats when contaminated.13
Although mask removal during walking around has been encouraged in the past; yet, it would be a sensible approach to regularly update the guidelines according to the current necessities.
Among the participants, 84.6% were trained regarding appropriate indications for hand hygiene and 82.5% confirmed the availability of supplies for a surgical hand scrub, but only 76.3% of them knew the proper duration for alcohol rub. Although the percentages seem reasonable; yet, the fact that 15.4% of the participants were unaware of the indications of hand hygiene emphasizes the need for more frequent and rigorous educational sessions. Educating the students about the adverse consequences of neglecting hand hygiene should go in parallel with providing all the necessary logistics.
Of the 240 surveyed subjects, 72.9% declared having a monitoring system for infection control practices, and 61.7% confirmed the availability of a sterilization monitoring system. Nonetheless, a study from Iraq revealed that only 32% of participating students checked the sterilization indicators.18 And a surprising result was revealed from India where 0% of the participants used indicators.19
These modest percentages draw attention to the gaps in attitude and practice that need to be dealt with. It is of crucial importance that dental students acknowledge the value of indicators and monitoring systems, and realize how defective monitoring can undermine their whole work.
On the other hand, vigilance regarding inhalational transmission is paramount for DHP. About 61.1% of our participants stated that the clinic offers instructions to patients with symptoms of respiratory infection, while 38.9% denied their knowledge. These percentages are not up to the standard, which implies that instructions and posters should be in more visible areas or even repeatedly depicted in different sites and different ways (text, pictures, and spoken words) in the clinic.
Out of the surveyed participants, 59.2% were recorded to clean blood spillage with alcohol, while 72.1% stated the availability of written recommendations regarding sharps disposal, and 73.3% confirmed the availability of instructions for handling contaminated reusable dental instruments. On the other hand, a study from Jordan revealed that 80.5% of participants asserted the presence of available protocol for sharps accidents.16 An earlier study from Egypt revealed even a higher percentage, where 97.2% of the students practiced safe sharps disposal. Given the low percentages in our study, the prevention of blood-borne accidents should be set as a priority in dental settings, together with rigorous training on post-exposure management.
Out of the surveyed participants, 75.8% revealed their intention to deal with patients suffering from infectious diseases, and 47.5% of participants stated that they had already dealt with them in the past. Compared to other studies, our results are considered above average. In a study by Assiri et al., 43.8% of participants expressed willingness to treat patients with infectious diseases and 15.1% said they previously dealt with them.13 Meanwhile, Al-Essa and AlMutairi reported that 66.7% of participants were willing to treat patients with infectious diseases, and 29.7% dealt with them in the past.20 Willingness to treat patients with infectious diseases is likely influenced by the confidence that health care providers have in their knowledge about infection control and in the training they had received. It is also a reflection of their confidence in the accessibility of necessary logistics and supplies.
Regarding environmental cleaning instructions, 75.8% of our participants approved the presence of a strategy for dealing with contaminated dental units, where 62.1% confirmed the presence of written instructions for surfaces disinfection. Corroborating our results, a study from Saudi Arabia demonstrated that 71.5% of participants admitted the application of surface disinfection between patients.21 On the other hand, a study from Pakistan revealed that 97.9% of students knew the importance of surface disinfection.17 These variations in the results may pertain to the existing policies and programs in different institutions. The lower percentages in our study underpin the need for spreading knowledge about disinfection on a wider scale and through various means to reach all students.
Concerning the water system, 72.5% of our participants accorded the availability of sterile water for irrigation, and 78.3% confirmed the routine flushing of the dental unit water lines. However, an earlier study revealed a lower percentage of participants (26.2%) who applied running water lines before starting treatment.22
Of our participants, 94.2% confirmed their willingness to conform to infection control measures in the future. Concordant with this result, Al-Essa and AlMutairi reported that 96% of their participants were willing to adopt the infection control measures,20 while Assiri et al. reported that 100% of participants confirmed their willingness.13 These high percentages infer that dental students probably don’t lack the motivation to commit. Hence, it is the role of the involved institutions to upgrade the students’ knowledge and training via well-coordinated continuous education.12 Clarifying the rationale of each procedure can further promote the students’ interest and compliance and even encourage them to educate others.
Of note, a limiting factor in our study was that it involved a single institution; hence, the results cannot be accurately generalized to all dental schools in Egypt. Nonetheless, the results can contribute to improving the educational strategies and designing tailored training policies.
The students’ knowledge about infection control practices was less than satisfactory. This necessitates prompt actions to design updated courses and programs, as well as a judicious approach that enthuses students to attend these courses. Prudent efforts should be exerted for training on the basic –yet crucial- procedures such as hand hygiene and the donning of PPE.
Meanwhile, a communication gap was noticeable where many students didn’t know about the availability of vaccines or various safety instructions. This mandates a corrective approach using up-to-date communication technologies. Successful communication would improve the students’ compliance with safety precautions till practicing these precautions becomes their norm in daily life.
In the same context, regular monitoring and serological tests for blood-borne viruses, e.g. HBV, should be encouraged and implemented on broad scales.
Further studies are warranted on larger sample sizes and in multiple institutions.
ACKNOWLEDGMENTS
We would like to express our sincere gratitude to students of ACU: Alaa G. Mohamed, Aliaa R. Fouad, Hoda M. El-Wawi, Sara M. Abdellah, Maria I. Nageeb, Nadin F. Diab, Amera I. Ibrahim, Diaa Essam-El-Deen, for their valuable efforts in collecting the data and assisting in analysis.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
All authors listed have made a substantial, direct, and intellectual contribution to the work, and approved it for publication.
FUNDING
None.
ETHICS STATEMENT
This study was approved by the Research Ethics Committee, Faculty of Medicine, Ahram Canadian University (ACU), Cairo, Egypt.
INFORMED CONSENT
Written Informed consent was obtained from the participants involved in the study.
AVAILABILITY OF DATA
All datasets generated or analyzed during this study are included in the manuscript.
- Yuzbasioglu E, Sarac D, Canbaz S, Sarac YS, Cengiz S. A Survey of Cross-Infection Control Procedures: Knowledge and Attitudes of Turkish Dentists. J Appl Oral Sci. 2009;17(6):565-569.
Crossref - Gopal S, Jesija JS, Vardhan BH. Cross Infection and Sterilization Methods: A Survey among Dental Practitioners in Chennai. International Journal of Contemporary Dental & Medical Reviews. 2014.
- Rahman B, Abraham SB, Alsalami AM, Alkhaja FE, Najem SI. Attitudes and Practices of Infection Control Among Senior Dental Students at College of Dentistry, University of Sharjah in the United Arab Emirates. Eur J Dent. 2013;7(S 01):S015-S019.
Crossref - Deogade SC, Suresan V, Galav A, Rathod J, Mantri SS, Patil SM. Awareness, Knowledge, and Attitude of Dental Students toward Infection Control in Prosthodontic Clinic of a Dental School in India. Niger J Clin Pract. 2018;21(5):553-559.
Crossref - Centers for Disease Prevention and Control (CDC). Recommendations from the Guidelines for Infection Control in Dental Health-Care Settings-2003. https://www.cdc.gov/oralhealth/infectioncontrol/pdf/recommendations-excerpt.pdf. Accessed 22 November 2021
- Ministry of Health and Population [Egypt], El-Zanaty and Associates [Egypt], and ICF International, Egyptian Demographic and Health Survey 2015. https://dhsprogram.com/pubs/pdf/FR313/FR313.pdf Accessed 22 November 2021
- Halboub ES, Al-Maweri SA, Al-Jamaei AA, Tarakji B, Al-Soneidar WA. Knowledge, Attitudes, and Practice of Infection Control among Dental Students at Sana’a University, Yemen. J Int Oral Health. 2015;7(5):15. PMID: 26028896
- Taiwo O. Dental practice, human immunodeficiency Virus Transmission and Occupational Risks: Views from a teaching hospital in Nigeria. Ann Med Health Sci Res. 2014;4(Suppl 2):S94-s98.
Crossref - Acosta-Gio AE, Borges Yanez SA, Flores M, et al. Infection Control Attitudes and Perceptions among Dental Students in Latin America: Implications for Dental Education. Int Dent J. 2008;58(4):187-193.
Crossref - Singh A, Purohit BM, Bhambal A, Saxena S, Singh A, Gupta A. Knowledge, attitudes, and Practice Regarding Infection Control Measures among Dental Students in Central India. J Dent Educ. 2011;75(3):421-427.
Crossref - El-saaidi C, Dadras O, Musumari PM, Ono-Kihara M, Kihara M. Infection Control Knowledge, Attitudes, and Practices among Students of Public Dental Schools in Egypt. Int J Environ Res Public Health. 2021;18(12):6248.
Crossref - Ravichandran RK, Jain J, Ananda SR, Jaduram B, Gunasekaran S. Knowledge, Attitude and Practices Regarding Hepatitis B and Infection Control among Clinical Dental Students. Int J Applied Dent Sci. 2019;5(3):42-46.
- Assiri KI, Kaleem SM, Ibrahim M, Alam T, Asif SM. Knowledge, Attitude, and Practice of Infection Control among Dental Students in King Khalid University, Abha. J Int Oral Health. 2018;10(2):83-87.
Crossref - Hbibi A, Kasouati J, Charof R, Chaouir S, El Harti K. Evaluation of the Knowledge and Attitudes of Dental Students toward Occupational Blood Exposure Accidents at the End of the Dental Training Program. J Int Soc Prev Community Dent. 2018;8(1):77-86.
- Abdelnaby A, Kamel LM, Elguindy J, Elamir RY, Elfar E. Exploring Safety Aspects in Dental School Clinics Including Droplet Infection Prevention. Open Access Macedonian Journal of Medical Sciences. 2020;8(E):509-515.
Crossref - Mahasneh AM, Alakhras M, Khabour OF, Al-Sa’di AG, Al-Mousa DS. Practices of Infection Control among Dental Care Providers: A Cross Sectional Study. Clin Cosmet Investig Dent. 2020;12:281-289.
Crossref - Qamar MK, Shaikh BT, Afzal A. What Do the Dental Students Know about Infection Control? A Cross-Sectional Study in a Teaching Hospital, Rawalpindi, Pakistan. BioMed Research International. 2020;2020:3413087.
Crossref - Fadil AG. Knowledge and Practice Regarding Infection Control among Dental Students at Basra University College of Dentistry, Iraq. International Journal of General Medicine and Pharmacy. 2016;5(6):35-46.
- Yadav BK, Rai AK, Agarwal S, Yadav B. Assessment of Infection Control Practice in private dental hospital. Int J Res Med Sci. 2017;5(11):4737-4742.
Crossref - AL-Essa NA, AlMutairi MA. To What Extent Do Dental Students Comply with Infection Control Practices? The Saudi Journal for Dental Research. 2017;8(1-2):67-72.
Crossref - Binalrimal S, AlDrees A, AlWehaibi M, et al. Awareness and Compliance of Dental Students and Interns toward Infection Control at Riyadh Elm University. GMS Hygiene and Infection Control. 2019;14.
Crossref - Mehta S, Mehta AJ, Lodha S. Study of Infection Control Procedures among Dental Clinics: A Pilot Study. J Interdiscipl Med Dent Sci. 2017;5(4):4.
Crossref
© The Author(s) 2021. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.