

ISSN: 0973-7510
E-ISSN: 2581-690X
Dengue is the most common and widespread arboviral infection in the world today. It is an increasingly prevalent tropical arbovirus infection with significant morbidity and mortality. Dengue fever is a recurrent problem in West Bengal. The purpose of this study is to present a comprehensive report on the diagnosis of Dengue fever cases with age and sex preponderance, data available from January 2013 to December 2016 at Malda Medical College, Malda, West Bengal. This is a cross-sectional investigative study done at Malda Medical College. In suspected Dengue fever cases, serum samples were tested for presence of Dengue NS1 antigen and presence of Dengue specific IgM antibodies by IgM antibody capture enzyme linked immunosorbent assay (MAC ELISA), strictly following the manufacturer’s protocol. On the year 2013, 2014, 2015 and 2016 Dengue confirmed cases were 25, 33, 68 and 1102 respectively. The number of Dengue cases in 2016 clearly outnumbered the Dengue cases in 2013, 2014 and 2015. In our study the highest numbers of cases were recorded in the age group 11 to 30 years and males were more affected than females. The majority of the cases were reported during the monsoon and post monsoon seasons. Dengue is increasing its geographical areas mostly everywhere now and this Dengue epidemiology demands efforts and support for controlling the disease effectively.
Dengue, 4 years analysis, Malda, West Bengal.
Dengue is the most common and widespread arboviral infection in the world today. It is an increasingly prevalent tropical arbovirus infection with significant morbidity and mortality.1 In recent times Dengue fever is getting attention in medical and social fields in developing countries especially in South East Asia.2 Presently, about 40% of the world’s population is at risk and there are 50 to 100 million cases every year. An estimated 500000 people with severe dengue require hospitalization each year and about 2.5% of those affected die.3According to WHO, nearly 75% of global burden of dengue fever are in south east regions and western pacific region.4Dengue infection has been known to be endemic in India for over two centuries.5 This emerging disease in India extending from urban area to semi urban and rural areas.4Dengue fever causes a major health, social and economic trouble on the populations of widespread areas.6Symptoms include fever, headache, retro orbital pain, muscle and joint pain and a characteristic skin rash, the disease may develops into the life threatening Dengue haemorrhagic fever (DHF) and Dengue shock syndrome (DSS).7 Dengue is transmitted mainly in India by Aedes aegypti mosquito and also by Aedes albopictus. Dengue fever is a recurrent problem in West Bengal.8 The purpose of this study is to present a comprehensive report on the diagnosis of Dengue fever cases with age and sex preponderance, data available from January 2013 to December 2016 at Malda Medical College, Malda, West Bengal.
This is a cross-sectional investigative study included the patients who attend the OPD (out patient department) and admitted in IPD (in patient department) of Malda Medical College, Malda with suspected cases of Dengue fever. Dengue fever patients typically develop sudden onset of high grade fever. Hence, fever cases of all age groups and either sex attending the (all the year round) Malda Medical College, were selected as per WHO criteria (An acute febrile illness with ≤2 of the following manifestations: headache, retro-orbital pain, myalgia, arthralgia, rash and haemorrhagic manifestation) and tested on referral microbiology laboratory, Department of Microbiology, Malda Medical College. Blood samples from suspected acute Dengue fever cases d” 4 days duration were tested for Dengue NS1 antigen and blood samples of suspected Dengue fever cases at least 5 days duration were tested for Dengue specific IgM by MAC ELISA test kit prepared by National Institute of Virology, Pune, India.
Serum samples were tested for presence of Dengue NS1 antigen and presence of Dengue specific IgM antibodies by IgM antibody capture enzyme linked immunosorbent assay (MAC ELISA), strictly following the manufacturer’s protocol.8, 9
Table 1 shows, on the year 2013, 72 fever cases were tested for Dengue NS1 Ag of which 7 cases were positive and 110 fever cases were tested for Dengue IgM Ab of which 18 cases were positive. Total confirmed cases were 25. Table 2 shows, out of 25 Dengue confirmed cases, 16 were male and 9 were female. Male:female ratio was 1.7:1. Table 3 shows, on the year 2014, 126 fever cases were tested for Dengue NS1 Ag of which 11 cases were positive and 202 fever cases were tested for Dengue IgM Ab of which 22 cases were positive. Total confirmed cases were 33. Table 4 shows, out of 33 Dengue confirmed cases, 23 were male and 10 were female. Male:female ratio was 2.3:1. Table 5 shows, on the year 2015, 125 fever cases were tested for NS1 Ag of which 9 cases were positive and 587 fever cases were tested for IgM Ab of which 59 cases were positive. Total confirmed cases were 68.Table 6 shows, out of 68 Dengue confirmed cases, 44 were male and 24 were female. Male: female ratio was 1.8:1. Table 7 shows, on the year 2016, 1859 fever cases were tested for NS1 Ag of which 433 cases were positive and 3216 fever cases were tested for IgM Ab of which 669 cases were positive. Total confirmed cases were 1102. Table 8 shows, out of 1102 Dengue confirmed cases, 652 were male and 450 were female. Male:female ratio was 1.4:1.
Table (1):
Dengue suspected and Positive cases on the year 2013.
Month |
Fever cases tested for Dengue NS1 Ag |
Dengue NS1 Ag ELISA Positive cases |
Fever cases tested for Dengue IgMAb |
Dengue IgM MAC ELISA Positive cases |
Total confirmed cases of Dengue |
|---|---|---|---|---|---|
January |
3 |
0 |
5 |
0 |
0 |
February |
1 |
0 |
4 |
0 |
0 |
March |
0 |
0 |
0 |
0 |
0 |
April |
0 |
0 |
0 |
0 |
0 |
May |
0 |
0 |
0 |
0 |
0 |
June |
8 |
0 |
12 |
1 |
1 |
July |
16 |
3 |
25 |
9 |
12 |
August |
15 |
2 |
21 |
3 |
5 |
September |
22 |
2 |
28 |
5 |
7 |
October |
7 |
0 |
12 |
0 |
0 |
November |
0 |
0 |
3 |
0 |
0 |
December |
0 |
0 |
0 |
0 |
0 |
Total |
72 |
7 |
110 |
18 |
25 |
Table (2):
Age and Sex wise distribution of Dengue confirmed cases on the year 2013.
| Dengue confirmed cases | |||
|---|---|---|---|
| Age (Years) | Male | Female | Total |
| 0-10 | 1 | 0 | 1 |
| 11-20 | 8 | 3 | 11 |
| 21-30 | 2 | 3 | 5 |
| 31-40 | 2 | 2 | 4 |
| 41-50 | 1 | 0 | 1 |
| 51-60 | 1 | 1 | 2 |
| >60 | 1 | 0 | 1 |
| Total | 16 | 9 | 25 |
Table (3):
Dengue suspected and Positive cases on the year 2014.
Month |
Fever cases tested for Dengue NS1 Ag |
Dengue NS1 Ag ELISA Positive cases |
Fever cases tested for Dengue IgMAb |
Dengue IgM MAC ELISA Positive cases |
Total confirmed cases of Dengue |
|---|---|---|---|---|---|
January |
1 |
0 |
6 |
0 |
0 |
February |
0 |
0 |
2 |
0 |
0 |
March |
0 |
0 |
0 |
0 |
0 |
April |
0 |
0 |
0 |
0 |
0 |
May |
0 |
0 |
3 |
1 |
1 |
June |
12 |
0 |
19 |
0 |
0 |
July |
14 |
1 |
26 |
3 |
4 |
August |
17 |
1 |
27 |
1 |
2 |
September |
24 |
2 |
31 |
3 |
5 |
October |
22 |
3 |
35 |
4 |
7 |
November |
28 |
4 |
42 |
10 |
14 |
December |
8 |
0 |
11 |
0 |
0 |
Total |
126 |
11 |
202 |
22 |
33 |
Table (4):
Age and Sex wise distribution of Dengue confirmed cases on the year 2014.
| Dengue confirmed cases | |||
|---|---|---|---|
| Age (Years) | Male | Female | Total |
| 0-10 | 3 | 2 | 5 |
| 11-20 | 2 | 2 | 4 |
| 21-30 | 4 | 3 | 7 |
| 31-40 | 8 | 1 | 9 |
| 41-50 | 5 | 1 | 6 |
| 51-60 | 1 | 0 | 1 |
| >60 | 0 | 1 | 1 |
| Total | 23 | 10 | 33 |
Table (5):
Dengue suspected and Positive cases on the year 2015.
Month |
Fever cases tested for Dengue NS1 Ag |
Dengue NS1 Ag ELISA Positive cases |
Fever cases tested for Dengue IgMAb |
Dengue IgM MAC ELISA Positive cases |
Total confirmed cases of Dengue |
|---|---|---|---|---|---|
January |
2 |
0 |
5 |
0 |
0 |
February |
0 |
0 |
2 |
0 |
0 |
March |
0 |
0 |
0 |
0 |
0 |
April |
0 |
0 |
0 |
0 |
0 |
May |
0 |
0 |
0 |
0 |
0 |
June |
0 |
0 |
3 |
0 |
0 |
July |
3 |
0 |
11 |
0 |
0 |
August |
16 |
0 |
27 |
3 |
3 |
September |
11 |
0 |
62 |
10 |
10 |
October |
0 |
0 |
242 |
18 |
18 |
November |
93 |
9 |
98 |
10 |
19 |
December |
0 |
0 |
137 |
18 |
18 |
Total |
125 |
9 |
587 |
59 |
68 |
Table (6):
Age and Sex wise distribution of Dengue confirmed cases on the year 2015.
| Dengue confirmed cases | |||
|---|---|---|---|
| Age (Years) | Male | Female | Total |
| 0-10 | 9 | 5 | 14 |
| 11-20 | 10 | 7 | 17 |
| 21-30 | 11 | 7 | 18 |
| 31-40 | 7 | 1 | 8 |
| 41-50 | 4 | 1 | 5 |
| 51-60 | 2 | 1 | 3 |
| >60 | 1 | 2 | 3 |
| Total | 44 | 24 | 68 |
Table (7):
Dengue suspected and Positive cases on the year 2016.
Month |
Fever cases tested for Dengue NS1 Ag |
Dengue NS1 Ag ELISA Positive cases |
Fever cases tested for Dengue IgMAb |
Dengue IgM MAC ELISA Positive cases |
Total confirmed cases of Dengue |
|---|---|---|---|---|---|
January |
0 |
0 |
21 |
3 |
3 |
February |
0 |
0 |
8 |
0 |
0 |
March |
0 |
0 |
0 |
0 |
0 |
April |
0 |
0 |
18 |
2 |
2 |
May |
0 |
0 |
8 |
0 |
0 |
June |
0 |
0 |
44 |
1 |
1 |
July |
0 |
0 |
55 |
6 |
6 |
August |
319 |
44 |
392 |
76 |
120 |
September |
284 |
61 |
509 |
102 |
163 |
October |
273 |
79 |
712 |
203 |
282 |
November |
445 |
120 |
1284 |
239 |
359 |
December |
538 |
129 |
165 |
37 |
166 |
Total |
1859 |
433 |
3216 |
669 |
1102 |
Table (8):
Age and Sex wise distribution of Dengue confirmed cases on the year 2016.
| Dengue confirmed cases | |||
|---|---|---|---|
| Age (Years) | Male | Female | Total |
| 0-10 | 86 | 76 | 162 |
| 11-20 | 200 | 113 | 313 |
| 21-30 | 171 | 94 | 265 |
| 31-40 | 85 | 86 | 171 |
| 41-50 | 53 | 47 | 100 |
| 51-60 | 41 | 28 | 69 |
| >60 | 16 | 06 | 22 |
| Total | 652 | 450 | 1102 |
The number of Dengue cases in 2016 clearly outnumbered the Dengue cases in 2013, 2014 and 2015. The highest numbers of cases were in the age group11 to 30 years with a male preponderance. The majority of cases during the months of august to December indicating increased vector transmission in the monsoon post monsoon periods.
Table 9 shows, analysis the risk factors of Dengue infection in total number of positive cases.
Table (9):
Analysis of Risk Factors in total number of positive cases (n= 1228).
| Risk Factors | ||||||
|---|---|---|---|---|---|---|
| Education | Illiterate | Primary | Upper primary | Secondary | Higher Secondary | Graduate |
| 612 | 361 | 102 | 90 | 41 | 22 | |
| Occupation | Student | Housewives | Unskilled labour | Skilled labour | Professional | Others |
| 94 | 42 | 656 | 408 | 20 | 08 | |
| Unhygienic environment around house | Present | Absent | ||||
| 1190 | 38 | |||||
| Indoor and Outdoor water containers to store water | Present | Absent | ||||
| 1228 | 0 | |||||
| Eliminate waters from artificial containers | Daily | Weekly | Monthly | |||
| 64 | 756 | 408 | ||||
| Screened doors and windows | Present | Absent | ||||
| 37 | 1191 | |||||
| Good air conditioning houses | Yes | No | ||||
| 88 | 1140 | |||||
| Using mosquito net | Yes | No | ||||
| 206 | 1022 | |||||
| Using mosquito repellents | Yes | No | ||||
| 0 | 1228 | |||||
| Wearing long-sleeved garments | Yes | No | ||||
| 97 | 1131 | |||||
| Activity around house | Yes | No | ||||
| 1186 | 42 | |||||
| Previous infection with a Dengue fever virus | Yes | No | ||||
| 22 | 1206 | |||||
Dengue is emerging as a major public health problem in India. It is one of the major public threats in West Bengal. The Dengue is gradually spreading to the rural areas of West Bengal.8 In our study, on the year 2013, 72 fever cases were tested for NS1 Ag of which 7 cases were positive and 110 fever cases were tested for IgM Ab of which 18 cases were positive. On the year 2014, 126 fever cases were tested for NS1 Ag of which 11 cases were positive and 202 fever cases were tested for IgM Ab of which 22 cases were positive. On the year 2015, 125 fever cases were tested for NS1 Ag of which 9 cases were positive and 587 fever cases were tested for IgM Ab of which 59 cases were positive. On the year 2016, 1859 fever cases were tested for NS1 Ag of which 433 cases were positive and 3216 fever cases were tested for IgM Ab of which 669 cases were positive. On the year 2013, 2014, 2015 and 2016 Dengue confirmed cases were 25, 33, 68 and 1102 respectively. The number of Dengue cases in 2016 clearly outnumbered the Dengue cases in 2013, 2014 and 2015. In our study the highest numbers of cases were recorded in the age group 11 to 30 years and males were more affected than females. This observation correlates with other studies.5, 8, 10, 11 The majority of the cases were reported during the monsoon and post monsoon seasons, in accordance with the reported patterns of Dengue transmission, that correlates with other studies.8,12,13,14 Analysis the risk factors of Dengue infection like unhygienic environment around house, indoor and outdoor water containers to store water and time taken for elimination of water, screened doors and windows, good air conditioning houses, using mosquito net and repellents, wearing long-sleeved garments etc. The finding of our study similar to other study.15, 16
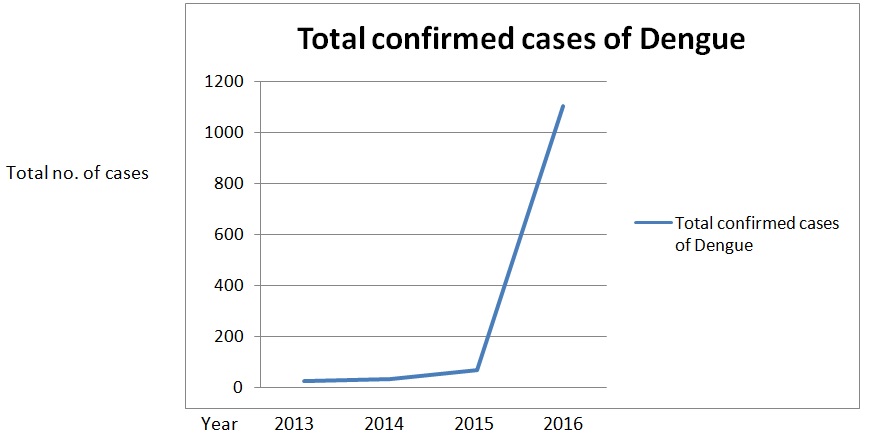
Fig. 1. Total confirmed cases of Dengue on the year 2013, 2014, 2015 and 2016
Dengue is a notifiable disease in India since 1996.7 Dengue is increasing its geographical areas mostly everywhere now and this Dengue epidemiology demands efforts and support for controlling the disease effectively. Dengue fever sometimes leads to death without proper treatment and care. There is no vaccine and specific drug to control infection but it is curable with proper symptomatic treatment and efforts.6 Attention is therefore required for effective vector control measures. Dengue infections are mostly seen in monsoon and post monsoon season, hence preventive measures should be in full swing at the early onset of monsoons.
- Gubler D J. Dengue and Dengue hemorrhagic fever. Clinical Microbiology Reviews. 1998; 11(3): 480-96.
- Bhatnagar S, Lal V, Gupta S D. Forecasting incidence of Dengue in Rajasthan. Indian Journal of Public Health. 2012; 56(4): 281-85.
- Cecilia D. Current status of Dengue and Chikungunya in India. WHO South-East Asia Journal of Public Health. 2014; 3(1): 22-27.
- Lal M, Aggarwal A, Oberoi A. Dengue fever- An emerging viral fever in Ludhiana, North India. Indian Journal of Public Health. 2007; 51(3): 198-99.
- Gupta E, Dar L, Kapoor G, Broor S. The changing epidemiology of Dengue in Delhi, India. Virology Journal. 2006; 3(4): 92-94
- Murugananthi C, Ramyachitra D. Dengue fever: an analysis. Indian Journal of Applied Research. 2014; 4(1): 155-57
- Gupta R, Tiwari R, Mueen A. Dengue research in India: A scientometric analysis of publications, 2003-12. International Journal of Medicine and Public health. 2014; 4(1) :1-8
- Bandyopadhyay B, Bhattacharya I et. al. A comprehensive study on the 2012 Dengue fever outbreak in Kolkata, India. Virology. 2013,Article ID 207580, 5 pages, http://dx.doi.org/10.5402/2013/207580
- Biswas T. Hemorrhagic stroke in Dengue; A rare sole presentation. International Journal of Innovative Research in Medical Sciences. 2016; 1(9): 395-98
- Chakravarti A, Kumaria R. Eco-epidemiological analysis of dengue infection during an outbreak of Dengue fever, India. Virology Journal. 2005; 2(32): 24-27
- Hati AK. Studies on Dengue and Dengue haemorrhagic fever (DHF) in West Bengal state, India. Journal of Communicable Diseases. 2006; 38(2): 124-29
- Reiter P. Climate change and mosquito borne disease. Environmental Health Perspectives. 2001; 109(1): 141-61
- University of Washington. Asia Pacific Emerging infection Network. Dengue.July 8, 2013. Available from: http://blogs.uw.edu/apecein/tag/dengue
- World Health Organisation. Dengue and severe dengue. Fact sheet no. 117, March 2014. Geneva: WHO, 2014. http://www.who.int/mediacentre/factsheets/fs117/en
- Chiou HY, Chao TY, Wang KJ. An investigation of the risk factors of a Dengue fever outbreak in Sanmin District, Kaohsiung City, 1998. Epidemiology Bulletin. 1999; 15(10): 173-188
- Ko YC, Chen MJ, Ye Sm. The predisposing and protective factors against Dengue virus transmission by mosquito vector. American Journal of Epidemiology. 1992; 136: 214-20.
© The Author(s) 2017. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.