


ISSN: 0973-7510
E-ISSN: 2581-690X
Urinary tract infection (UTI) poses a serious health issue for all age groups from neonates to geriatric age groups. Majority of the women experience urinary tract infections once in their lifetime. Escherichia coli (E.coli) is the most common uropathogen causing UTI which is followed by Klebsiella and Enterococci. Amoxicillin is the most resistant antibiotic against both E.coli and Klebsiella pneumonia whereas Gentamycin and Nitrofurantoin have been sensitive to both E.coli and Klebsiella pneumonia. Gram-negative bacteria such as E. coli, Klebsiella species, Proteus species, Acinetobacter species, Enterobacter species, Pseudomonas aeruginosa, and Citrobacter species are the most common causes of UTI. Enterococcus species, Staphylococcus saprophyticus, and Coagulase-negative bacteria are among Gram-positive bacteria. Staphylococcus aureus is a coagulase-positive gram-positive bacteria that cause urinary tract infections (UTIs). Hence, we come to the serious conclusion that Uropathogens are becoming increasingly resistant to a different group of antibiotics. The misuse and indiscriminate use of antimicrobials have led to the emergence of antibiotic resistance in bacteria all over the world, posing a threat to the public. Estimating the local etiology and sensitivity pattern could help in successful treatment. Inquiring into UTI epidemiology, such as risk factors, bacterial strains, and antimicrobial susceptibility, could help healthcare planners determine the best course of action.
Antibiotic Susceptibility, CAUTI, Nosocomial Infection, UPEC, Urinary Tract Infection, Uropathogens
Urinary tract infection (UTI) is the most frequent bacterial infection that causes patients to seek medical attention. Approximately 10% of people will develop a urinary tract infection (UTI) at some point in their lives.1 UTIs are also the most common infection associated with hospitals and healthcare. In comparison to male urethras, female urethras are shorter and are located near the perirectal region. After the age of 60, the risk of UTI in men increases as the prostate enlarges and interferes with the clearance of urine from the bladder. In females, the incidence of bacteriuria steadily rises over time.2 The link between UTIs and sexual activity may potentially play a role in the increased occurrence. Changes in anatomical structure, as well as hormonal changes, grows the threat of bacteriuria during pregnancy, which leads to a growing threat of UTI. The most common cause of simple UTI is E. coli. UPEC causes UTIs that are distinct from other UTIs at the molecular level.3 Other bacteria that cause urinary tract infections include Klebsiella, Enterobacteriaceae, Staphylococcus saprophyticus, Enterococci, and others. The relative prevalence of infection caused by Proteus, Pseudomonas, Klebsiella, and Enterobacteriae spp. increases in complicated UTIs. Furthermore, community-acquired UTIs are becoming increasingly linked to multidrug-resistant pathogens such as beta-lactamase-resistant E. coli.4 E. coli, Klebsiella, Proteus spp., Staphylococci, Pseudomonas aeruginosa, Enterobacter spp., and Candida spp. are the most common bacteria found in hospitalized patients (Table). ESBL, Beta-lactamase, Carbapenemase-producing Enterobacteriaceae, and Acinetobacter spp. are becoming more common in healthcare-associated UTIs.5 Gram-negative bacteria like Acinetobacter spp., Pseudomonas spp., Gardnerella vaginalis, and others are less typically isolated species. Immunocompromised patients, such as those who have had a renal transplant, are not only prone to conventional uropathogens, but also to opportunistic infections with uncommon pathogens. For example, urine specimens from renal transplant patients may include Listeria monocytogenes, which are linked to systemic illness.6 During the early stages of typhoid illness, Salmonella spp. might be recovered. Candida spp. has been isolated from immunocompromised patients with diabetes and other diseases. Systemic infections can be caused by fungi such as Blastomyces dermatitidis, Cryptococcus neoformans, and others. Viruses and parasites do not have a role in UTI development.7 Haemorrhagic cystitis in children, on the other hand, is thought to be caused by adenovirus. Trichomonas vaginalis can be found in urine sediment on rare occasions. The three forms of infection are ascending, hematogenous, and lymphatic. The ascending route is the usual source of infection in women.8 Instrumentation used in healthcare, such as urinary catheterization, cystoscopy, and other procedures, causes UTIs in both men and women. Bacteria can be propelled into the bladder via the urethra and then move down the track within the catheter and the urethral mucosa, gaining access to the bladder. Hematogenous or blood-borne UTIs are also possible. Bacteraemia is the most repeated reason for hematogenous spread. Seeding of the kidney can occur with any systemic infection, but with specific species, such as Staph. Aureus or Salmonella, are more invasive. Hematogenous spread accounts for more than 5% of UTIs and happens only rarely with gram-negative bacteria.9 Finally, increasing bladder pressure might result in lymphatic movement into the kidneys, resulting in a UTI. Because urine has a low PH, a high or low osmolality, a high urea content, or a high organic acid content, microbes that are resistant to antibiotics thrive in it. The mucosal surfaces of the bladder also have antibacterial characteristics. As a result, if the infection is not completely cleared, the infection site will remain on the superficial mucosa, with deep layers of the bladder rarely being affected.10 In addition, a valve-like mechanism at the ureter-bladder junction prevents urine from the bladder from refluxing into the upper urinary tract. Urine reflux provides a direct channel for organisms to reach the kidney if valve function is hindered by obstruction or congenital abnormalities. Urine reflux to the urinary system is increased by hormonal changes linked with pregnancy and their impact on the urinary tract. Uropathogens activate the human immunological response, which aids in the fight against infection.11 Contact of bacteria with urothelial cells. Through a number of signaling mechanisms, it triggers an immunological response. Bacterial lipopolysaccharide stimulates the release of cytokines such as tumor necrosis factor (TNF) and Interferon-gamma by activating host cells. Bacteria can also activate the complement cascade, which results in the creation of physiologically active components like opsonin.12 In the current situation, where antibiotic resistance patterns are rapidly changing and novel MDR bacteria are regularly appearing, morbidity and mortality are increasing. According to the European Survey of Antibiotic Consumption, multidrug-resistant (MDR) bacteria are the reason for the deaths of over 25,000 Europeans each year, most of whom die as a result of complications from UTIs. The Infectious Diseases Society of America suggests that geographical inspection be carried out to track changes in uropathogenic sensitivity in certain areas.13
Table :
Name of uropathogens.
| Gram-Positive Organisms | Gram-Negative Organisms |
|---|---|
| Enterococcus spp. | Escherichia coli |
| Staphylococcus aureus | Proteus mirabilis |
| Staphylococcus saprophyticus | Klebsiella pneumoniae |
| Streptococcus spp. | Pseudomonas aeruginosa |
| Enterobacter cloacae | |
| Providencia spp. | |
| Morganella morganii | |
| Serratia spp. | |
| Citrobacter spp. |
Pathophysiology
The link between uropathogens and host characteristics is poorly understood. Generally, E. coli is the most frequent uropathogen. Because of intrinsic or extrinsic urinary tract abnormalities, complicated UTIs are becoming more common in the elderly population. Complex UTIs are those that arise among immunosuppression patients, such as diabetes, or the presence of anatomical or functional abnormalities of the urinary tract.14 Uropathogens use a variety of virulence factors and pathogenic processes to colonize and infect the urinary system. The release of ammonia causes the pH of urine to rise, allowing urinary ions to precipitate in the form of crystals. Stones in the kidneys or bladder can induce Proteus infection. Another avenue for colonization of the urinary system is biofilm development, which is particularly crucial for stones and other foreign materials.15 “Uncomplicated” infections originated in a normal genitourinary tract with no prior instrumentation, whereas “complicated” infections are identified in the genitourinary tract with anatomical or functional abnormalities, covering equipment like catheters, Copper – T, and so on.16 The most common uropathogen associated with the development of UTI is Uropathogenic Escherichia coli (UPEC). UPEC colonizes the bladder via a variety of virulence factors that play a key role in Urinary tract infection pathogenesis (Figure 2).17 The great larger part of Uropathogenic Escherichia coli collected from female patients with acute, asymptomatic, or recurring UTIs has flagellum-mediated motility. In an iron-deficient environment like the urinary system, the survival rate of UPEC is low as the iron acquisition is difficult. UTIs are most frequently seen in the bladder. UPEC commonly bypasses BECs and the bladder epithelium, despite their features. The urethra becomes polluted as bacteria colonize the intestines, and the infection usually starts there.18 The bladder epithelium is divided into 3 layers: a basal cell layer, an intermediate cell layer, and a superficial apical layer having diameters of 5-10 m, 20 m, and 25–250 m respectively, referred to as “umbrella cells” (Figure 1). A basement membrane lies beneath the basal epithelium. Umbrella cells act an important role in protecting the body from the majority of toxins contained in urine.19

Figure 1. Structure of Urinary Tract and bacterial invasion through it
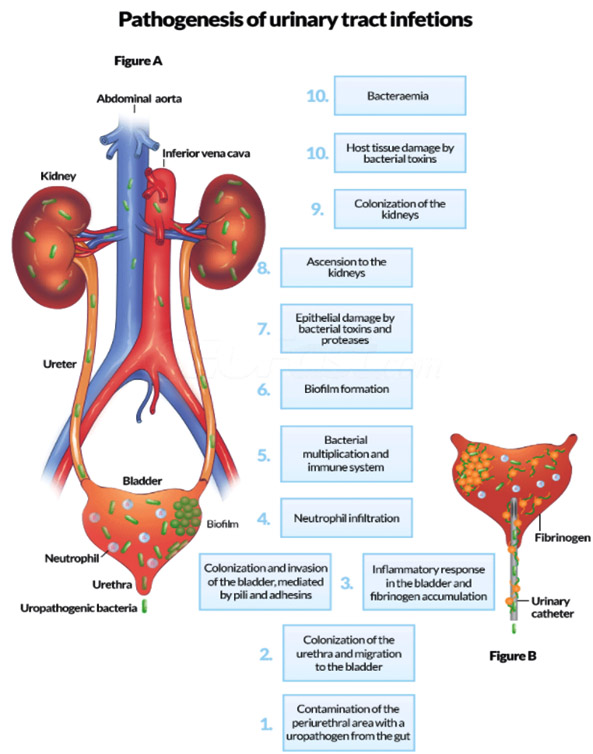
Figure 2. Pathogenesis of UTI
Immunological Aspects of MDR
Several chemotherapeutic drugs, including daunorubicin, vincristine, and colchicine, are resistant to multidrug resistance (MDR), which is caused, in part, by the overexpression of P-glycoprotein.20 A P-glycoprotein overexpressing variation of the HL60 myeloid leukemia cell line is known as RV+ cells. In addition to showing conventional MDR, RV+ cells showed relative resistance to cytotoxicity caused by immunoglobulin G and M antibodies against several cell surface antigens, but not to cytotoxicity caused by antibodies alone or to killing brought on by lymphokines.21 Verapamil therapy and particular monoclonal antibodies (mAbs) that can bind to P- glycoprotein and disrupt its action were both effective in reversing complement resistance. Further evidence is that the selection of the cells on vincristine did not lead to the resistance of RV+ cells. Investigations were conducted on a second system using P-glycoprotein-infected agents. The MDR1 gene-infected K562 cells, which were not subjected to chemotherapeutic drug selection, also showed some resistance to complement-mediated cytotoxicity.22 Monoclonal antibodies that bind to P-glycoprotein were also effective in reversing this MDR1 infection-induced resistance. As a result, the P- glycoprotein-mediated MDR phenotype confers resistance to complement-mediated cytotoxicity. The MDR phenotype’s higher intracellular pH and lower membrane potential may cause aberrant membrane attack complex function. This finding may have ramifications for P-potential glycoprotein’s modes of action as well as its potential physiological function in preventing complement-mediated autolysis.23
Methods
Peer-reviewed articles were searched and referred for the uropathogens causing urinary tract infections. Articles from the past three decades were considered which include PubMed, Scopus, and Google Scholar. A review template was developed to extract information from the literature identified for the structured literature review.
A community bacterial UTI is the most common reason which needs attention for medical treatment. The most frequent aetiological agent causing UTI is Escherichia coli, which accounts for up to 90% of cases.24 The analysis showed that the antibiotic resistance rate is greater than a frequently used antibiotic. Amoxicillin resistance was reported in Escherichia coli and K. pneumoniae organisms, which is a very significant antibiotic. In the other case antibiotics like ceftriaxone, nitrofurantoin, and gentamycin exhibited very low levels of resistance, and past research in other countries found a similar percentage of sensitivity for these drugs.25 Finally, uropathogens with increased antibiotic resistance were identified. When it comes to selecting a drug for empirical UTI treatment, practitioners have limited options due to the finding of uropathogens are highly resistant to different common antibiotics.26 As a result, doctors and other field health workers must be reminded that empiric UTI treatment must be re-evaluated. There are two approaches to treating UPEC infections: directly and indirectly.27 Indirect techniques stimulate infected tissues for taking action against UPEC invasion, eliciting and enhancing immune responses. Direct techniques target bacteria viability, bladder epithelial adherence, and biofilm development; indirect techniques stimulate infected tissues and increase immune responses.28 It’s not impossible that new treatments will contain both antimicrobials and natural substances. According to a growing amount of research, reducing UPEC adhesion to urinary tract tissues helps reduce recurrence and improve health. Bacteria that cause UTIs have more aggressive virulence factors than non-pathogenic bacteria, which boost their host cell adhesion, colonization, and invasion abilities.29 To avoid being identified by the host’s immune system, these bacteria use virulence factors, which are made up of cell components like pili, capsules, lipopolysaccharides, and different surface features.30 Anatomical and physiological factors of humans, such as the urethra’s shorter length, contribute to an increased risk of UTI. Similarly, insufficient bladder emptying, particularly in the elderly, leads to the accumulation of leftover urine.31
Complex UTIs are those that arise with immunosuppressive, such as in diabetic patients, or in the presence of a defective urinary tract. As the population ages, complicated UTIs, which can be caused by abnormal urinary tract, are gradually increasing.32 Intrinsic abnormalities such as congenital deformities, a neurogenic bladder, and urinary fistulae are examples of intrinsic abnormalities that may raise the risk of UTI. Stents and catheters are examples of extrinsic abnormalities that can cause UTIs.33 Uropathogens use a variety of virulence factors and pathogenic processes to colonize and infect the urinary system. Urease, an enzyme that hydrolyses urea (CH4N2O) to NH3 and CO2, is produced by several uropathogens, particularly Proteus spp. The ammonia release increases the pH of the urine, promoting kidney or bladder stones, that may lead to P. mirabilis infection.34 The other avenue for colonization in the urinary system is biofilm development, which is particularly crucial for stones and other foreign materials.35 P. aeruginosa is recognized for its propensity to form biofilms, thanks to genes like alginase, which are essential for the biofilm’s exopolysaccharide matrix formation.36 Antibiotic resistance mechanisms, like vancomycin-resistant enterococci and Klebsiella pneumoniae with ESBL enzyme, are common in nosocomial UTIs. Among nosocomial infections, catheter-associated urinary tract infection (CAUTI) is the most common, which consists of 40% of all.37,38
ACKNOWLEDGMENTS
The authors would like to thank Department of Microbiology of the Institute of Medical Sciences & SUM Hospital, Bhubaneswar, Odisha, India, and the Dean of IMS & SUM Hospital, SOA, Bhubaneswar, India for their support.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORS’ CONTRIBUTION
MD and BB Conceptualized and designed the study. PB performed literature review. MD, BB, BR and RP performed data acquisition. MD and BB wrote the manuscript. MD, BB, BR, RP and PB reviewed and edited the manuscript. All authors read and approved the final manuscript for publication.
FUNDING
None.
DATA AVAILABILITY
Not applicable.
ETHICS STATEMENT
Not applicable.
- Barisic Z, Babic-Erceg A, Borzic E, Zoranic V, Kaliterna V, Carev M. Urinary tract infections in South Croatia: aetiology and antimicrobial resistance. Int J Antimicrob Agents. 2003;22(Suppl 2):61-64.
Crossref - Beyene G, Tsegaye W. Bacterial uropathogens in urinary tract infection and antibiotic susceptibility pattern in jimma university specialized hospital, southwest ethiopia. Ethiop J Health Sci. 2011;21(2):141-146.
Crossref - Ahmed SS, Shariq A, Alsalloom AA, Babikir IH, Alhomoud BN. Uropathogens and their antimicrobial resistance patterns: Relationship with urinary tract infections. Int J Health Sci. 2019;13(2):48-55. PMID: 30983946
- Ravishankar U, Sathyamurthy P, Thayanidhi P. Antimicrobial Resistance Among Uropathogens: Surveillance Report From South India. Cureus. 2021;26;13(1):e12913.
Crossref - Seifu WD, Gebissa AD. Prevalence and antibiotic susceptibility of uropathogens from cases of urinary tract infections (UTI) in Shashemene referral hospital, Ethiopia. BMC Infect Dis. 2018;18(1):30.
Crossref - Sefton AM. The impact of resistance on the management of urinary tract infections. Int J Antimicrob Agents. 2000;16(4):489-491.
Crossref - Bonadio M, Meini M, Spitaleri P, Gigli C. Current microbiological and clinical aspects of urinary tract infections. Eur Urol. 2001;40(4):439-445.
Crossref - Amalaradjou MA, Narayanan A, Venkitanarayanan K. Trans-cinnamaldehyde decreases attachment and invasion of uropathogenic Escherichia coli in urinary tract epithelial cells by modulating virulence gene expression. J Urol. 2011;185(4):1526-1531.
Crossref - Ronald AR, Nicolle LE, Stamm E, et al. Urinary tract infection in adults: research priorities and strategies. Int J Antimicrob Agents. 2001;17(4):343-348.
Crossref - Beerepoot MA, Geerlings SV, Van Haarst EP, Van Charante NM, Ter Riet G. Nonantibiotic prophylaxis for recurrent urinary tract infections: a systematic review and meta-analysis of randomized controlled trials. J Urol. 2013;190(6):1981-1989.
Crossref - Bien J, Sokolova O, Bozko P. Role of uropathogenic Escherichia coli virulence factors in the development of urinary tract infection and kidney damage. Int J Nephrol. 2012;2012:681473.
Crossref - Wilson ML, Gaido L. Laboratory diagnosis of urinary tract infections in adult patients. Clin Infect Dis. 2004;38(8):1150-1158.
Crossref - Crude N, Tveten Y, Kristiansen BE. Urinary tract infections in Norway: bacterial etiology and susceptibility. A retrospective study of clinical isolates. Clin Microbiol Infect. 2001;7(10):543-547.
Crossref - Aubron C, Glodt J, Matar C, et al. Variation in endogenous oxidative stress in Escherichia coli natural isolates during growth in urine. BMC Microbiol. 2012;12:120.
Crossref - Lee DS, Lee SJ, Choe HS. Community-Acquired Urinary Tract Infection by Escherichia coli in the Era of Antibiotic Resistance. Biomed Res Int. 2018; 2018:7656752.
Crossref - Bielecki P, Muthukumarasamy U, Eckweiler D, et al. In vivo mRNA profiling of uropathogenic Escherichia coli from diverse phylogroups reveals common and group-specific gene expression profiles. MBio. 2014;5(4): e01075-14.
Crossref - Ghosh A, Bandyopadhyay D, Koley S, Mukherjee M. Uropathogenic Escherichia coli in India an Overview on Recent Research Advancements and Trends. Appl Biochem Biotechnol. 2021;193(7):2267-2296.
Crossref - Terlizzi ME, Gribaudo G, Maffei ME. UroPathogenic Escherichia coli (UPEC) infections: virulence factors, bladder responses, antibiotic, and non-antibiotic antimicrobial strategies. Front Microbiol. 2017;8:1566.
Crossref - Wiles TJ, Kulesus RR, Mulvey MA. Origins and virulence mechanisms of uropathogenic Escherichia coli. Exp Mol Pathol. 2008;85(1):11-19.
Crossref - Weisburg JH, Curcio M, Caron PC, et al. The multidrug resistance phenotype confers immunological resistance. J Exp Med. 1996;183(6):2699-2704.
Crossref - Handel A, Margolis E, Levin BR. Exploring the role of the immune response in preventing antibiotic resistance. Journal of Theoretical Biology. 2009;256(4):655-662.
Crossref - Abraham SN, Miao Y. The nature of immune responses to urinary tract infections. Nat Rev Immunol. 2015;15(10):655-663.
Crossref - Aguiniga LM, Yaggie RE, Schaeffer AJ, Klumpp DJ. Lipopolysaccharide domains modulate urovirulence. Infect Immun. 2016;84(11):3131-3140.
Crossref - Bishop BL, Duncan MJ, Song J, Li G, Zaas D, Abraham SN. Cyclic AMP-regulated exocytosis of Escherichia coli from infected bladder epithelial cells. Nat Med. 2007;13(5):625-630.
Crossref - Blango MG, Mulvey MA. Persistence of uropathogenic Escherichia coli in the face of multiple antibiotics. Antimicrob Agents Chemother. 2010;54(5):1855-1863.
Crossref - Cai W, Wannemuehler Y, Dell’Anna G, et al. A novel two-component signaling system facilitates uropathogenic Escherichia coli‘s ability to exploit abundant host metabolites. PLoS Pathog. 2013;9(6):e1003428.
Crossref - Haque R, Akter M, Salam M. Prevalence and susceptibility of uropathogens: a recent report from a teaching hospital in Bangladesh. BMC Res Notes. 2015;8(1):416.
Crossref - Petca RC, Mares C, Petca A, et al. Spectrum and antibiotic resistance of uropathogens in Romanian females. Antibiotics. 2020;9(8):472.
Crossref - Ahmad M, Kumar P, Sultan A, Akhtar A, Chaudhary B, Khan F. Prevalence of Community-Acquired Uropathogens and their Antimicrobial Susceptibility in Patients from the Urology Unit of A Tertiary Care Medical Center. J Pure Appl Microbiol. 2020;14(3):2009-2015.
Crossref - Dasgupta C, Rafi MA, Salam MA. High prevalence of multidrug-resistant uropathogens: A recent audit of antimicrobial susceptibility testing from a tertiary care hospital in Bangladesh. Pak J Med Sci. 2020;36(6):1297-1302.
Crossref - Govindarajan DK, Kandaswamy K. Virulence factors of uropathogens and their role in host-pathogen interactions. The Cell Surf. 2022;8:100075.
Crossref - Kranz J, Schmidt S, Lebert C, Schneidewind L, Schmiemann G, Wagenlehner F. Uncomplicated Bacterial Community-Acquired Urinary Tract Infection in Adults. Dtsch Arztebl Int. 2017;114(50):866-873.
Crossref - Ognenovska S, Mukerjee C, Sanderson-Smith M, Moore KH, Mansfield KJ. Virulence Mechanisms of Common Uropathogens and Their Intracellular Localisation within Urothelial Cells. Pathogens. 2022;11(8):926.
Crossref - McLellan LK, Hunstad DA. Urinary tract infection: pathogenesis and outlook. Trends Mol Med. 2016;22(11):946-957.
Crossref - Andersen TE, Khandige S, Madelung M, et al. Escherichia coli uropathogenesis in vitro: invasion, cellular escape, and secondary infection analyzed in a human bladder cell infection model. Infect Immun. 2012;80(5):1858-1867.
Crossref - Cegelski L, Pinkner JS, Hammer ND, et al. Small-molecule inhibitors target Escherichia coli amyloid biogenesis and biofilm formation. Nat Chem Biol. 2009;5(12):913-919.
Crossref - Letica-Kriegel AS, Salmasian H, Vawdrey DK, et al. Identifying the risk factors for catheter-associated urinary tract infections: a large cross-sectional study of six hospitals. BMJ Open. 2019;9(2):e022137.
Crossref - Cortese YJ, Wagner VE, Tierney M, Devine D, Fogarty A. Review of catheter-associated urinary tract infections and in vitro urinary tract models. J Healthc Eng. 2018;2018:2986742.
Crossref
© The Author(s) 2022. Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License which permits unrestricted use, sharing, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.